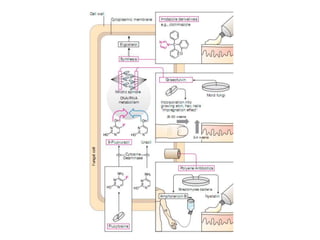
This document discusses antifungal drugs used to treat fungal infections. It covers several classes of antifungals including polyenes like amphotericin B and nystatin that damage fungal cell membranes, azoles like fluconazole and itraconazole that inhibit ergosterol synthesis, echinocandins like caspofungin that inhibit cell wall synthesis, and other antifungals such as flucytosine and allylamines. Each drug's mechanism of action, indications, dosage, administration route, efficacy, side effects, and drug interactions are described. The document provides an in-depth overview of antifungal drug properties and use in treating various fungal diseases