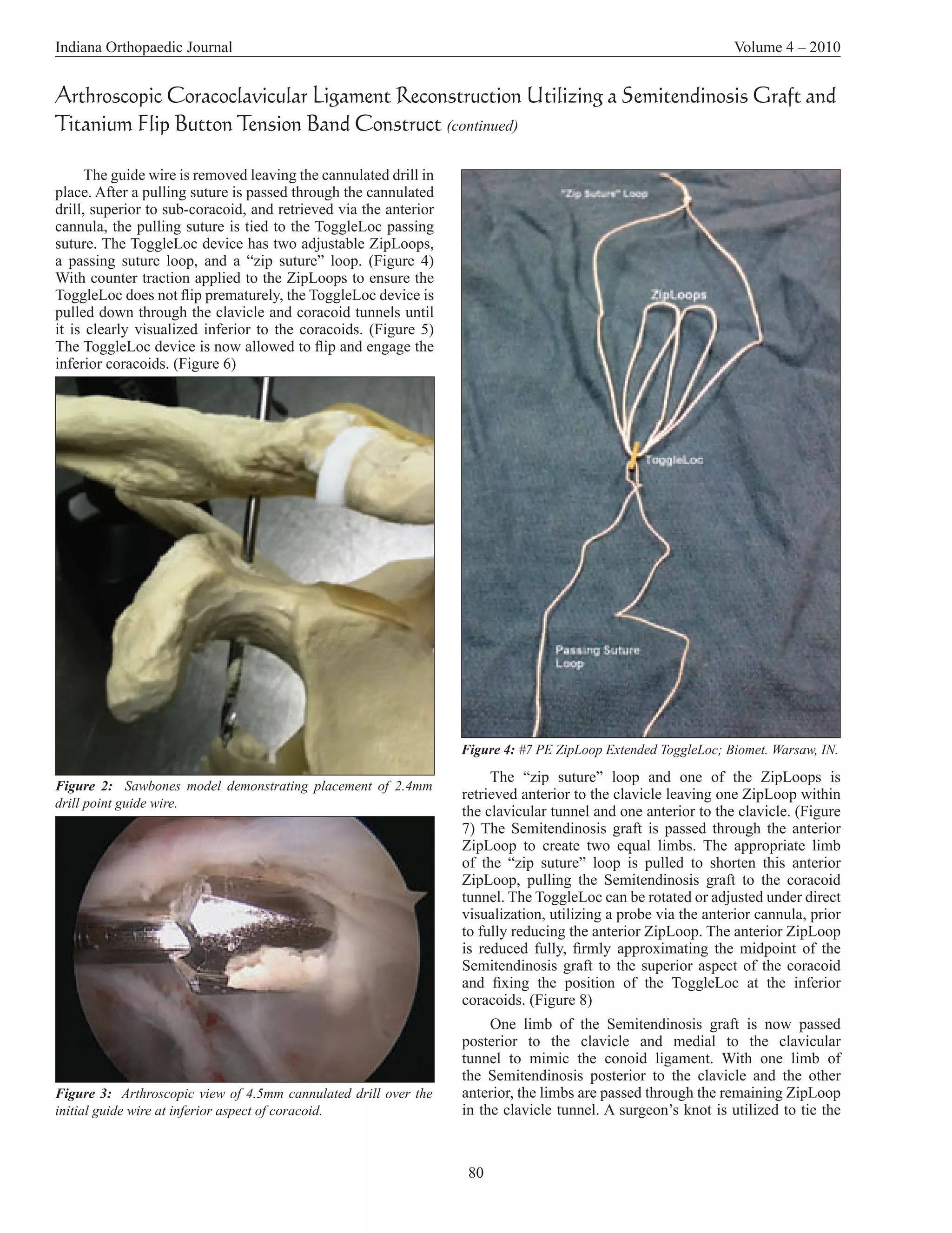
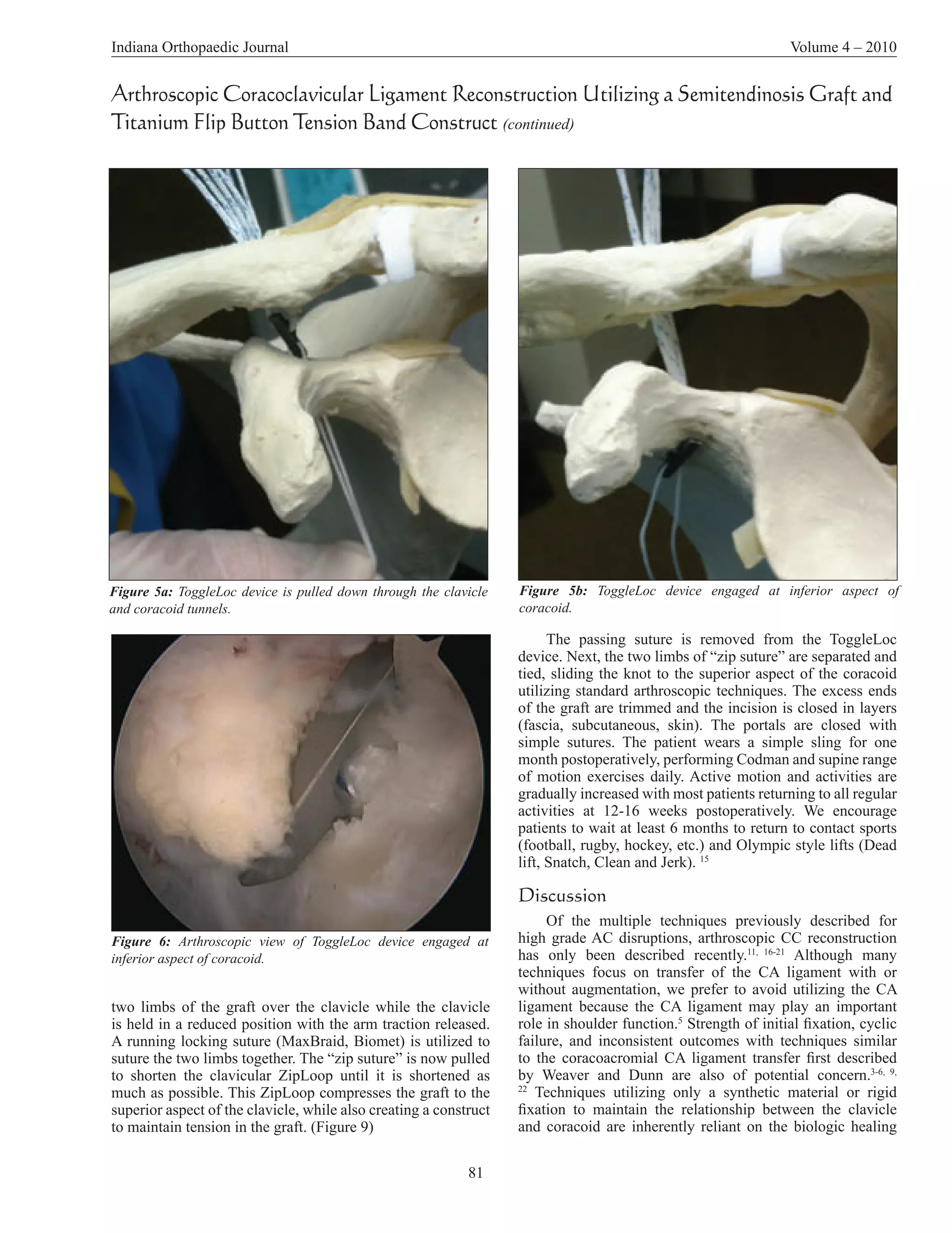
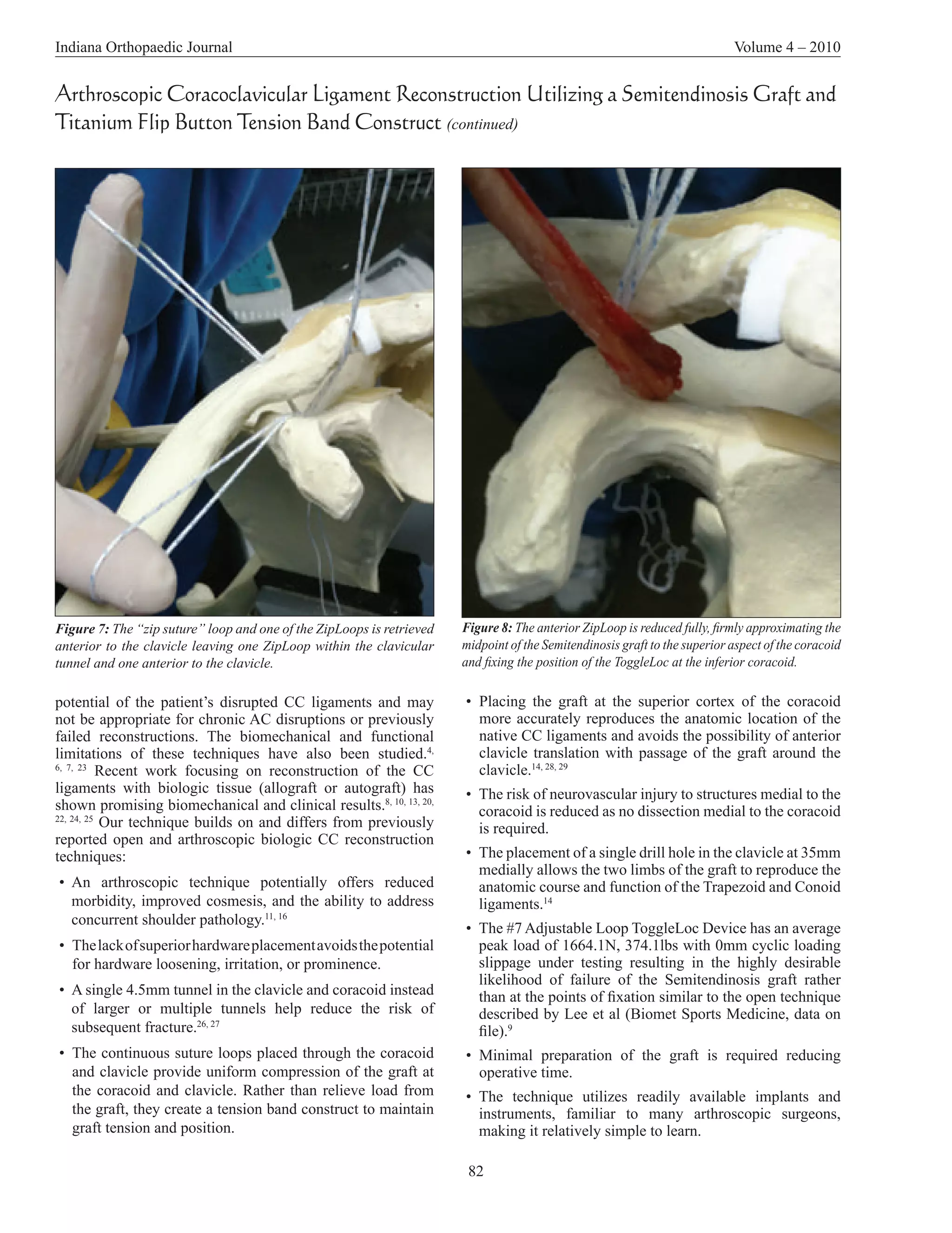
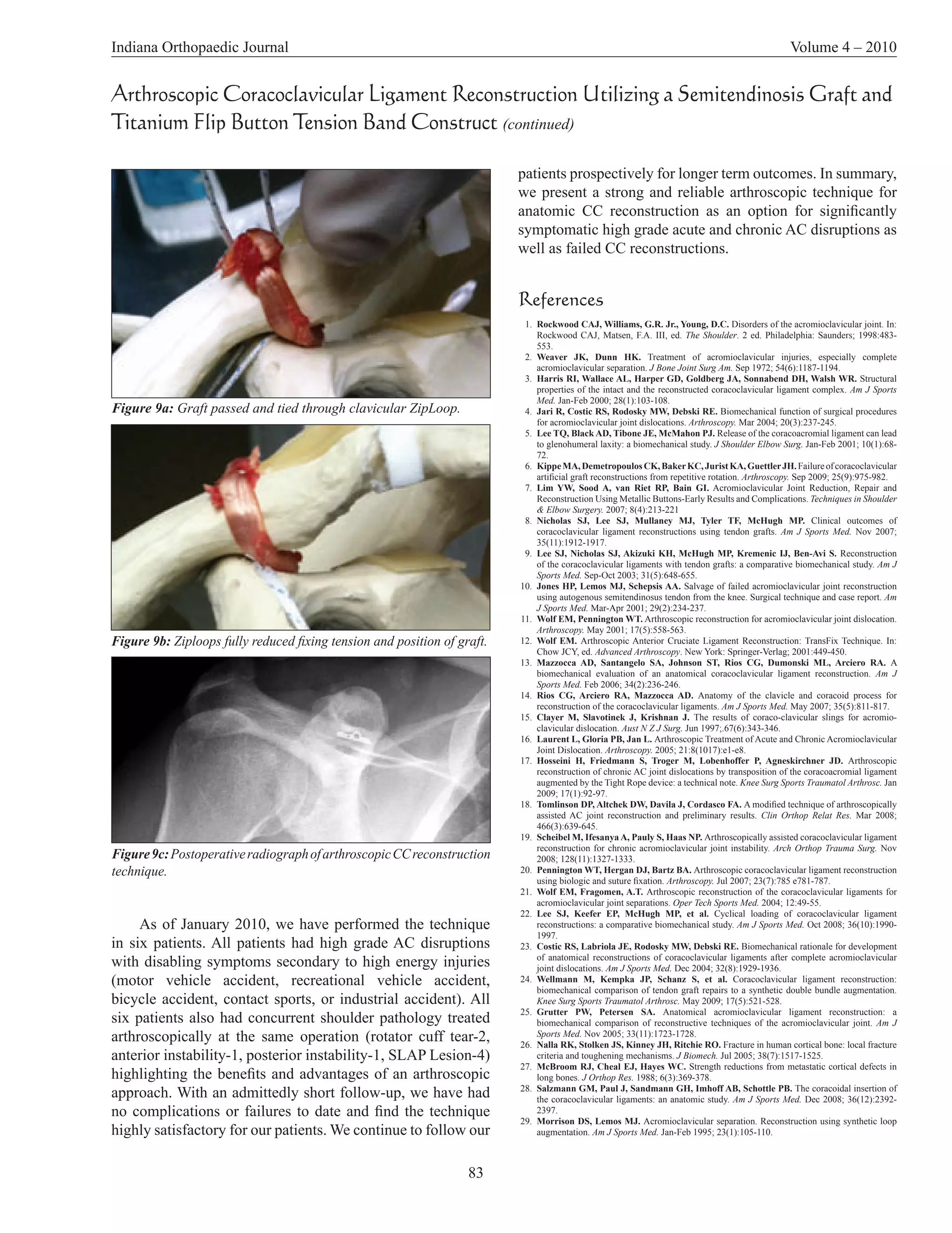
This document describes an arthroscopic technique for reconstructing the coracoclavicular (CC) ligaments using a semitendinosus graft and titanium flip button tension band construct. The technique involves drilling tunnels in the clavicle and coracoid process, passing the graft and flip button through the tunnels, and securing the graft with suture loops to reconstruct the CC ligaments. Compared to previous techniques, this method aims to more accurately reproduce the anatomy, avoid hardware issues, and provide strong initial fixation with minimal morbidity. The technique offers an arthroscopic option for treating symptomatic AC joint disruptions that builds on past open and arthroscopic reconstruction methods.