1) Abdominal pain in children can be caused by many common and age-specific issues like intussusception in infants and appendicitis in older children.
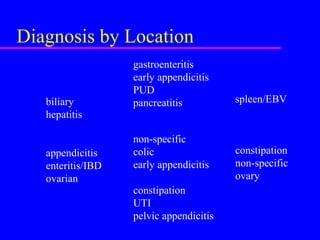
2) A thorough history and physical exam are important for diagnosing the cause, with location and timing of pain providing clues. Common surgical issues include appendicitis, intussusception, and incarcerated hernias.
3) Further testing like bloodwork, imaging, and observation may be needed to determine if urgent surgery is required for problems like a perforated viscus or uncontrolled bleeding, or if the issue can be monitored as a potential "medical bellyache".