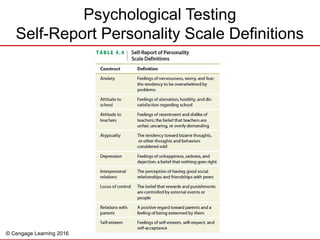
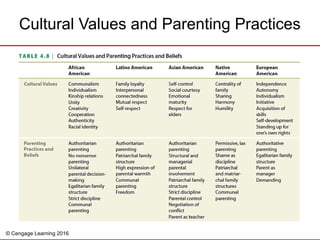
The document outlines clinical assessment, diagnosis, and treatment approaches for children with psychological disorders, emphasizing the importance of understanding individual and cultural contexts. It discusses idiographic and nomothetic formulation, various assessment methods, and the pros and cons of diagnostic labels. Treatment strategies are highlighted, with a focus on evidence-based interventions tailored to cultural needs and the necessity of addressing family dynamics and ethical considerations in the therapeutic process.







![History clinical assessment[1]](https://cdn.slidesharecdn.com/ss_thumbnails/history-clinicalassessment1-110821092905-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































![Behavior[1]](https://cdn.slidesharecdn.com/ss_thumbnails/4c474616-c8d5-42a1-b869-31f6136d3bcc-150623100548-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![Psychodiagnostic technique[1]](https://cdn.slidesharecdn.com/ss_thumbnails/psychodiagnostictechnique1-191031121907-thumbnail.jpg?width=640&height=640&fit=bounds)





















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
