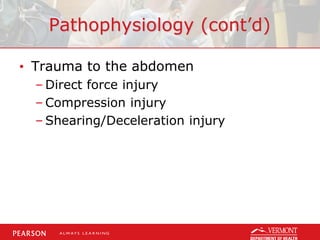
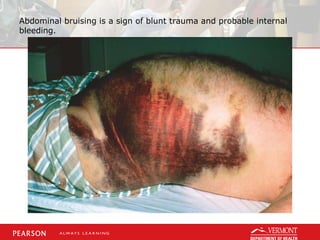
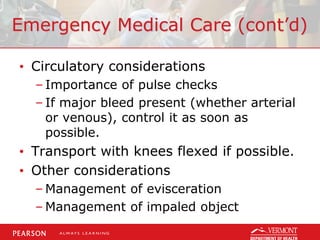
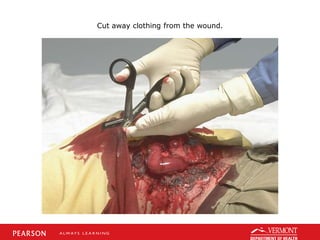
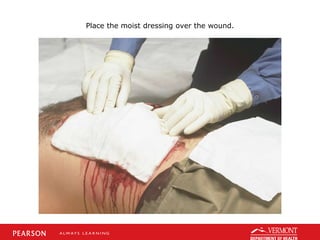
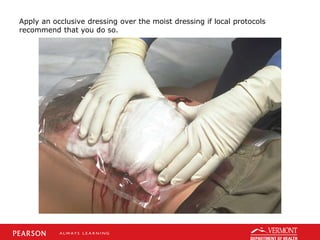
This document discusses pathophysiology of abdominal trauma, assessment findings depending on the injured abdominal quadrant, emergency medical care including considerations for airway, circulation, and transport, and a case study of a patient kicked in the abdomen by a horse. Key details include types of abdominal injuries from direct force, compression, or shearing; signs of internal bleeding like abdominal pain, guarding, distention, or shock; managing the patient's airway, circulation, and injuries on scene; and providing oxygen, immobilization, and rapid transport to the hospital for someone with possible liver damage from a horse kick.




























































![제 23회 보아즈(BOAZ) 빅데이터 컨퍼런스 - [MBOAX] : ABSA를 활용한 소비자 반응 분석 기반 운영 효율화 대시보드 설계](https://cdn.slidesharecdn.com/ss_thumbnails/3-1boaz23rdconferencemboax-260203102709-9d519923-thumbnail.jpg?width=640&height=640&fit=bounds)
![7.__Developing_a_Research_Proposal[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/7-260131073037-df92dd7d-thumbnail.jpg?width=640&height=640&fit=bounds)





![Hacking-Uncovered-How-People-Get-Hacked-and-How-to-Stay-Safe[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hacking-uncovered-how-people-get-hacked-and-how-to-stay-safe1-260130170011-4883a9c7-thumbnail.jpg?width=640&height=640&fit=bounds)