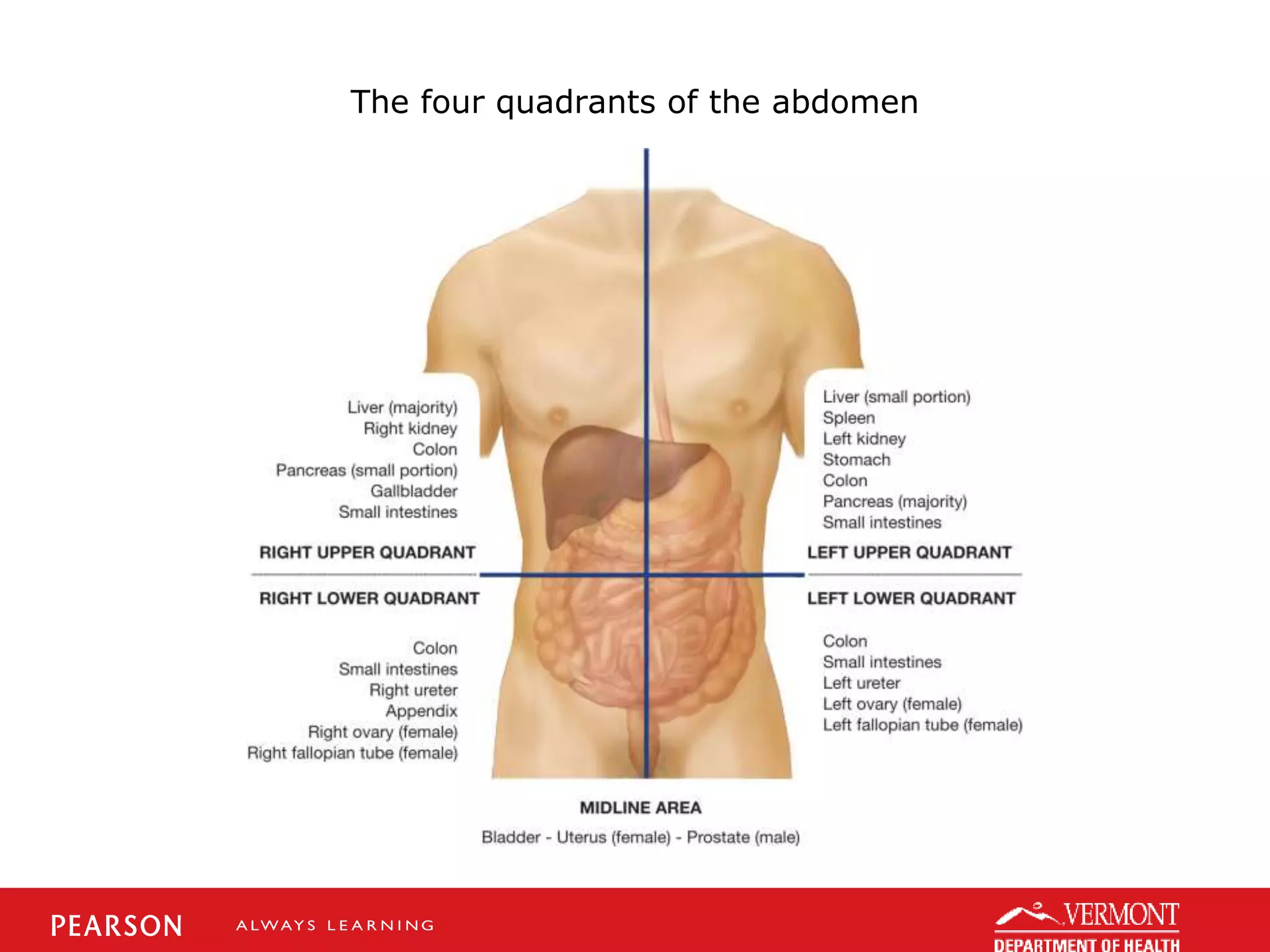
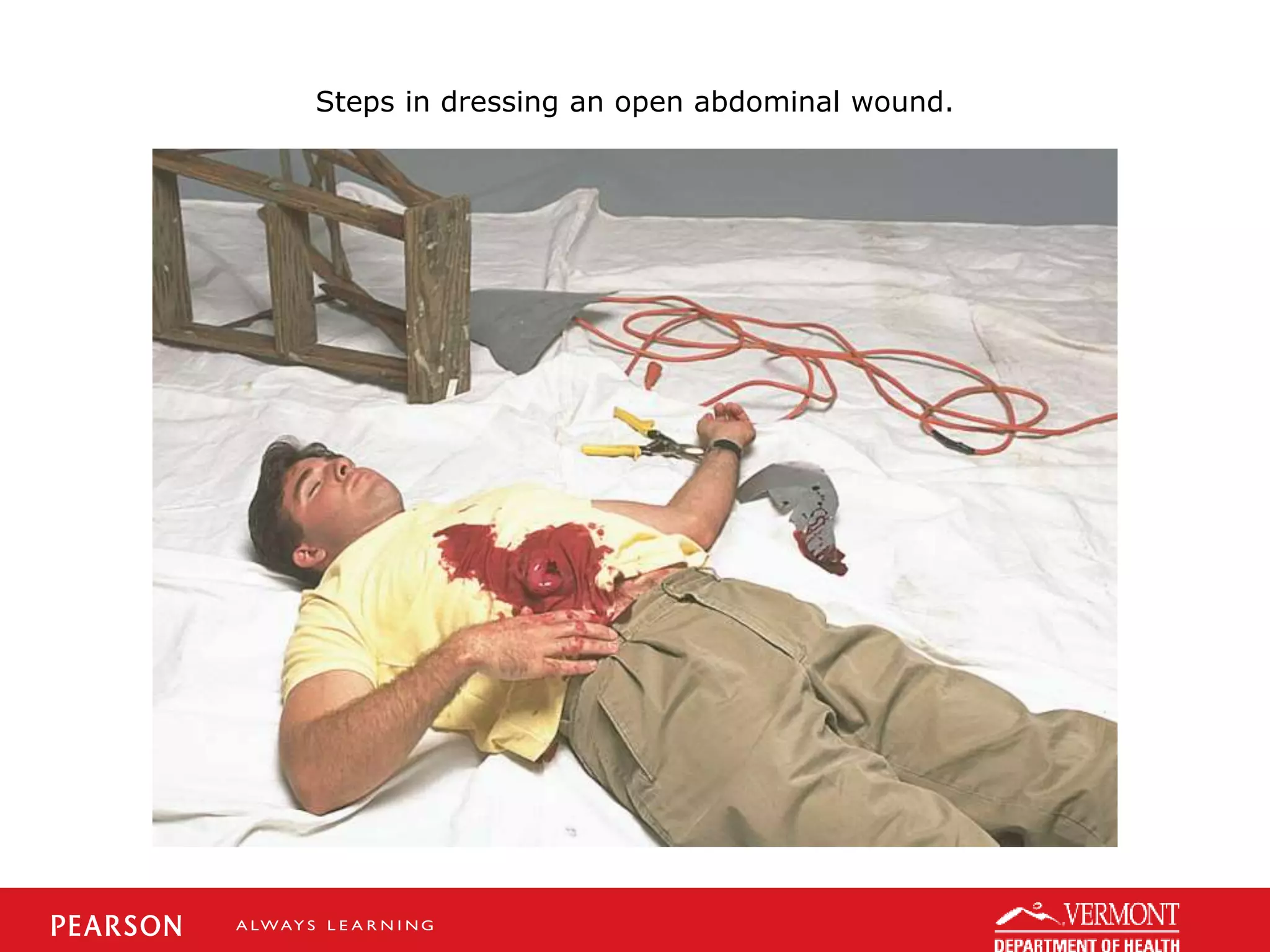
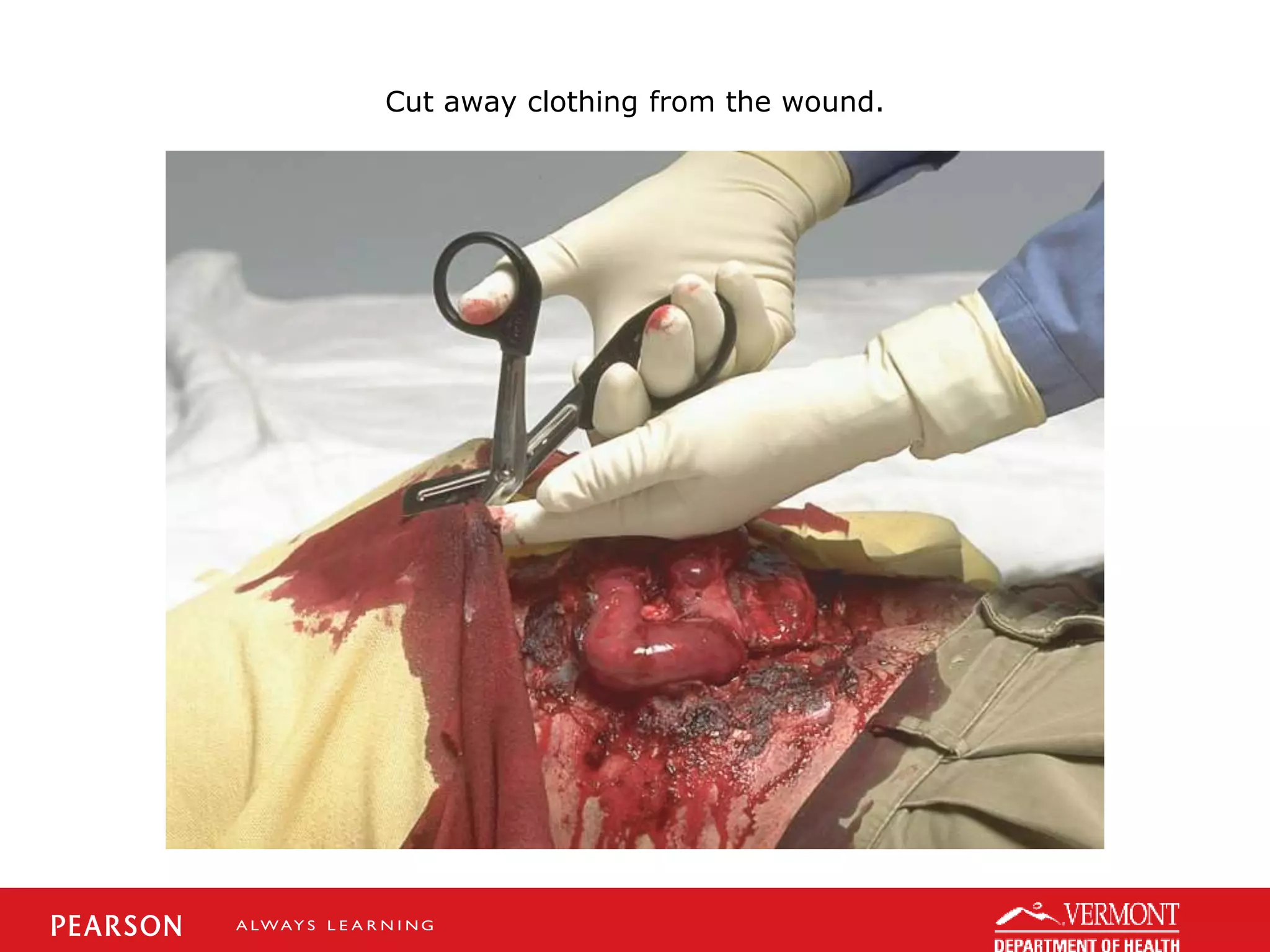
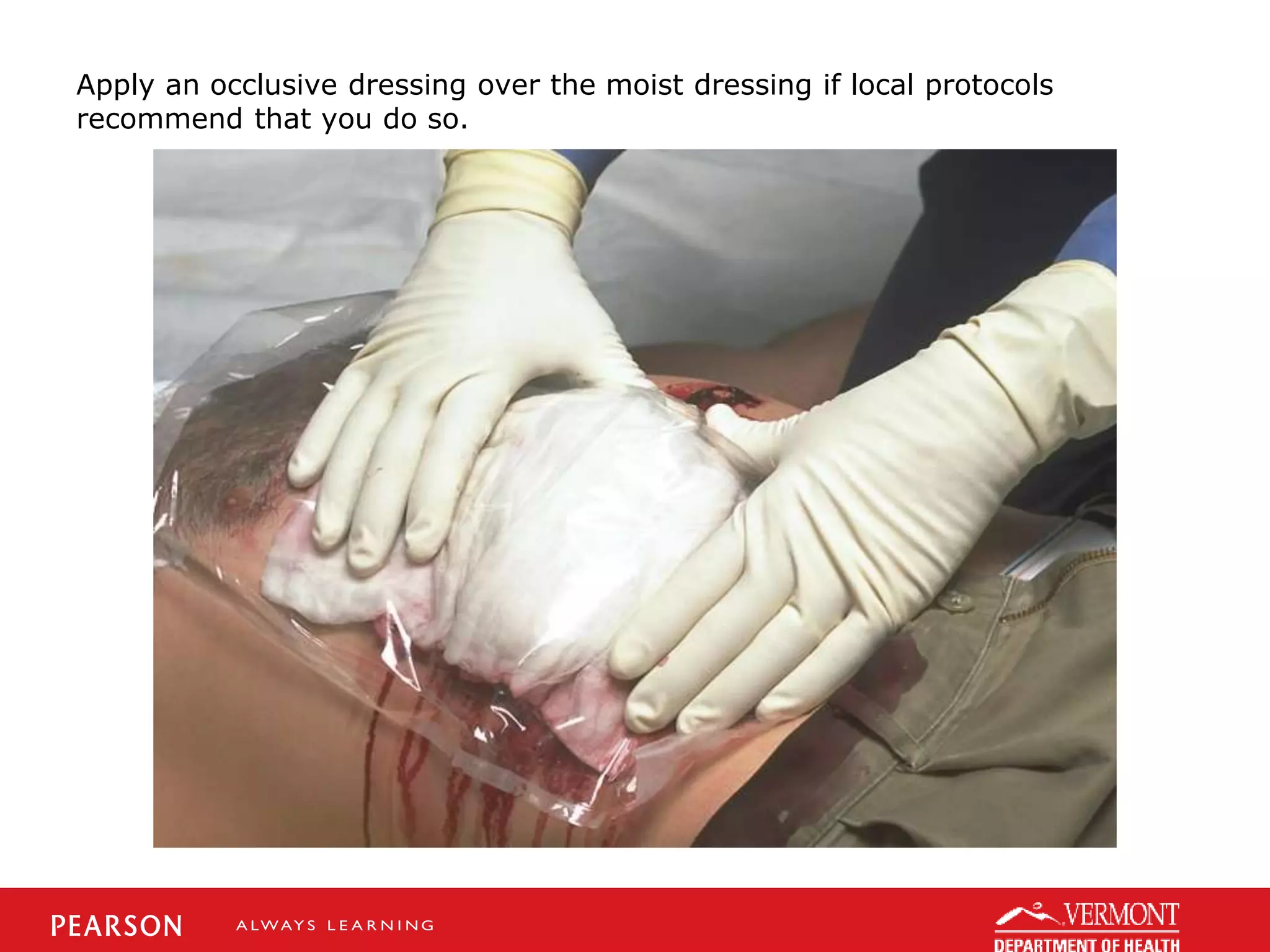
Abdominal trauma can cause internal bleeding and injury to organs. Assessment findings may include abdominal pain, bruising, guarding, or shock. Treatment includes spinal immobilization, airway support, bleeding control, and rapid transport. The case study describes a patient kicked in the abdomen who is tachycardic and in abdominal pain, indicating potential liver injury requiring high priority care and transport.