A Randomised Controlled Study to VIsualise improvement in (1).pptx
1.
A RANDOMISED CONTROLLEDSTUDY TO VISUALISE
IMPROVEMENT IN MUCOSAL VISIBILITY DURING UPPER
GASTROINTESTINAL ENDOSCOPY AFTER PREMEDICATION WITH
A COMBINATION OF SIMETHICONE AND N-ACETYL CYSTEINE
Presenter: Dr. Abhiram M Gogi
Mentors: Dr. Prem Kumar
Dr. Sunil Kumar
Dr. Srinivas NM
Dr. Kemparaj T
2.
Introduction
▪ Esophagogastroduodenoscopy isone of the most commonly performed endoscopic procedure which
provides valuable information in patients with upper gastrointestinal (GI) conditions 1
.
▪ Gastric cancer is the fifth leading cause of cancer in the world and the third leading cause of cancer-
related death2
.
▪ Endoscopic diagnosis of early gastric cancer is difficult because it often shows only subtle changes
on endoscopic examination, and requires good endoscopic technique, with optimum preparation of
patients 3
.
▪ Many studies have been done in East Asian countries where premedication with simethicone and
pronase or N-acetylcysteine was used to improve mucosal visualization during upper endoscopy6-8
.
MCM- SSBASICC- BMCRI- 18/09/2024
3.
3
Aims & Objectives
▪To assess the improvement in mucosal visualisation in upper GI endoscopy after premedication
with a combination of simethicone and N- acetyl cystein using a novel specifically designed scoring
system.
MCM- SSBASICC- BMCRI- 18/09/2024
4.
4
Methodology
▪ A prospective,endoscopist blinded, randomized study enrolled patients who underwent
esophagogastroduodenoscopy in a single center where patients were randomized to receive or not
receive an oral preparation with simethicone and N-acetylcysteine in water.
▪ The sample size was calculated as approximately 50 in each group. (case and control)
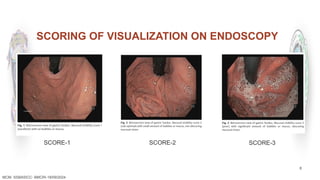
▪ A preset scoring system where a score of 1 to 3 score was assigned to each part and visualization
was graded by using a specific, previously arranged scale, namely esophagus, fundus, body, antrum
and duodenum so that the total score ranged from 5 to 15 .
▪ Time between endoscope insertion and clean achievement (mouth to clean time) and the end of
examination (mouth to mouth time) was recorded.
MCM- SSBASICC- BMCRI- 18/09/2024
5.
MCM- SSBASICC- BMCRI-21/09/2022 5
▪ INCLUSION CRITERIA
▪ Male and Female <18 yrs to 60 yrs>
▪ Dyspepsia
▪ Gastroesophageal reflux disease
▪ Chronic liver disease for evaluation of portal hypertension
▪ Anemia
▪ Unexplained weight loss
▪ Chronic diarrhea
▪ Recurrent vomiting
▪ EXCLUSION CRITERIA
▪ On going upper GI bleed
▪ Hypersensitivity to semithacone or NAC
▪ Pregnant and lactating females
▪ Previously operated cases
▪ Corrosive intake/viral/fungal etiology
▪ Unwilling to provide informed written consent
▪ Esophageal stricture or gastric outlet obstruction
▪ Previous upper gastrointestinal surgery
▪ Severe cardiorespiratory illness
6.
MCM- SSBASICC- BMCRI-21/09/2022 6
▪ Pre endoscopic preparation
▪ The patients were randomly assigned to receive (case group) or not (control group) a preparation,
with allocation ratio 1:1.
▪ The premedication was prepared by dissolving a combination of simethicone and 600mg NAC
dissolved in 45mL of water as prepared by a nurse and was orally administered 20 minutes before
endoscopy to patients.
▪ Controls underwent endoscopy without pre-endoscopic preparation.
7.
7
MCM- SSBASICC- BMCRI-18/09/2024
▪ Mucosal scoring
▪ Two skilled endoscopists blinded to the premedication performed the endoscopies and graded visualization by
using a specific, previously arranged scale.
▪ A score of 1 to 3 score was assigned to each part namely esophagus fundus, body, antrum and duodenum so that
the total score ranged from 1 to 15 .
▪ The participating endoscopists examined a set of 20 images corresponding to different degrees of mucosal
visualisation, and scores were discussed until agreement was reached and the interobserver agreement was
calculated using the Kappa statistic.
▪ For each examination, time between the insertion of the endoscope and the achievement of a clean stomach
(mouth to clean time) and the end of the examination (mouth to mouth time) were also recorded.
▪ The amount of water needed to achieve optimal mucosal visualization, and the number of times suction was
used was recorded as well.
9
▪ Stastical analysis:
▪The collected data was analysed with IBM.SPSS statistics software 23.0 Version.
▪ To describe about the data descriptive statistics frequency analysis, percentage analysis was used
for categorical variables and for continuous variables the mean and S.D was used.
▪ Kolmogorov – Smirnov test and kurtosis, skewness was used to test the normality of the data (50 <
n > 300).
▪ To find the association of significance in categorical data the Chi-Square test was used.
▪ Student t test was used to compare continuous variables.
▪ In all the above statistical tools the probability value .05 will be considered as significant level.
MCM- SSBASICC- BMCRI- 18/09/2024
10.
10
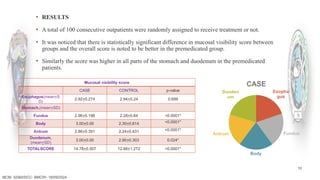
▪ RESULTS
▪ Atotal of 100 consecutive outpatients were randomly assigned to receive treatment or not.
▪ It was noticed that there is statistically significant difference in mucosal visibility score between
groups and the overall score is noted to be better in the premedicated group.
▪ Similarly the score was higher in all parts of the stomach and duodenum in the premedicated
patients.
MCM- SSBASICC- BMCRI- 18/09/2024
Mucosal visibility score
CASE CONTROL p-value
Esophagus(mean+S
D)
2.92+0.274 2.94+0.24 0.699
Stomach,(mean+SD)
Fundus 2.96+0.198 2.28+0.64 <0.0001*
Body 3.00+0.00 2.30+0.614 <0.0001*
Antrum 2.86+0.351 2.24+0.431 <0.0001*
Duodenum,
(mean+SD)
3.00+0.00 2.90+0.303 0.024*
TOTALSCORE 14.78+0.507 12.66+1.272 <0.0001*
Esopha
gus
Fundus
Body
Antrum
Duoden
um
CASE
11.
11
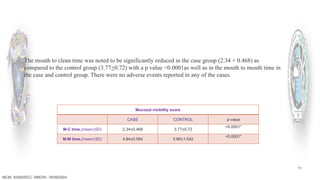
Mucosal visibility score
CASECONTROL p-value
M-C time,(mean+SD) 2.34+0.468 3.77+0.72
<0.0001*
M-M time,(mean+SD) 4.84+0.584 5.66+1.042
<0.0001*
MCM- SSBASICC- BMCRI- 18/09/2024
The mouth to clean time was noted to be significantly reduced in the case group (2.34 + 0.468) as
compared to the control group (3.77+0.72) with a p value <0.0001as well as in the mouth to mouth time in
the case and control group. There were no adverse events reported in any of the cases.
12.
12
Results
▪ The overallscore is noted to be better in the premedicated group.
▪ The mucosal visibility score was higher in all parts of the stomach and duodenum in them.
▪ The mouth to clean time was noted to be significantly reduced in the prepared patients as compared
to the control group .
▪ However there was no significant difference in the mouth to mouth time in the premedicated and
control group indicating a greater amount of time being spent in observing gastric mucosa in the
premedicated patients.
MCM- SSBASICC- BMCRI- 18/09/2024
13.
13
Discussion
MCM- SSBASICC- BMCRI-18/09/2024
▪ For better visualization of the gastric mucosa, decreasing the amount of mucus and bubbles is very
important during UGI endoscopy.
▪ Adequate premedication can eliminate the need to carry out flushing during the procedure.
▪ Optimizes the efficiency of most of our endoscopy units that are understaffed and overburdened.
▪ Preparation is easily available, cheap, convenient to administer, well tolerated, and very effective.
▪ Time taken for UGIE would also differ between operators and indications; hence, it might not be an
ideal representation.
▪ The mucosal visibility in every individual patient prior to pre-medication to assess the impact of
individual preparations could not be compared.
14.
14
Conclusions
▪ Premedication withsimethicone and NAC resulted in better mucosal visibility and improve
diagnostic yield, hence should be considered for standard practice.
MCM- SSBASICC- BMCRI- 18/09/2024
15.
15
References
▪ Cohen J,Safdi MA,DealSEetal.Quality indicators for esophagogastroduodenoscopy.Am.J.Gastroenterol.2006;101:886–91.
▪ BrayF, FerlayJ ,Soerjomataram I etal.Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality world wide for 36 cancers in 185 countries. CA:ACancer Journal
for Clinicians2018;68:394–424
▪ Dinis-Ribeiro M, Areia M, de Vries A Cetal. Management of precancerous conditions and lesions in the stomach(MAPS): guideline from the European Society of Gastrointestinal
Endoscopy(ESGE), European Helicobacter Study Group(EHSG), European Society of Pathology(ESP), and the Sociedade Portuguesade Endoscopia
Digestiva(SPED).Endoscopy2012;44:74–94
▪
Yao K. The endoscopic diagnosis of early gastric cancer. Ann Gastroenterol2013;26:11–22
▪ Faigel D O, Eisen G M,Baron T Hetal. Preparation of patients for GI endoscopy. Gastrointest Endosc2003;57:446–450
▪ Chang WK, Yeh MK, Hsu HCetal .Efficacy of simethicone and N-acetylcysteine as premedication in improving visibility during upper endoscopy: premedication before
upperendoscopy. J GastroenterolHepatol2014;29:769–774
▪ Asl SM,Sivandzadeh GR.Efficacy of premedication with activated Dimethicone or N-acetylcysteine in improving visibility during upper endoscopy. World J
Gastroenterol2011;17:4213–4217
▪ Chang C-C, Chen S-H, LinC-Petal. Premedication with pronase or Nacetyl cysteine improves visibility during gastroendoscopy: anendoscopist-blinded, prospective, randomized
study.World J Gastroenterol2007;13:444–447
▪ Manfredi G, Bertè R, Iiritano E, Alicante S, Londoni C, Brambilla G, Romeo S, Menozzi F, Griffanti P, Brandi G, Moreschi O, Pezzilli R, Zullo A, Buscarini E. Premedication with
simethicone and N-acetylcysteine for improving mucosal visibility during upper gastrointestinal endoscopy in a Western population. Endosc Int Open.2021Feb;9(2):E190-E194.
▪ Elvas L, Areia M, Brito Detal. Premedication with simethicone and Nacetylcysteine in improving visibility during upperendoscopy: a double-blind randomized
trial.Endoscopy2016;49:139–145
▪ Anikhindi SA ,Kumar A, Uedo N, Singla V, Anikhindi A, Sharma P,etal. Pre-Endoscopy Drink of Simethicone and N-Acetylcysteine Significantly Improves Visualization in Upper
Gastrointestinal Endoscopy. Journal of Digestive Endoscopy.2021Mar;12(01):011–8.
MCM- SSBASICC- BMCRI- 18/09/2024
17
Delete this slide
▪Add slides in between as u require
▪ 7 lines per slide
▪ Avoid full sentences- Just type in keywords
▪ Add pictures and charts- Don’t type the explanation but don’t forget to explain.
▪ Do not read the slides, Speak/ Explain
▪ If u are running short of time, Skip the discussion and directly come to
conclusions and end it in time.
▪ Address the President/ Secretary SSBASIC and HOD BMCRI
MCM- SSBASICC- BMCRI- 21/09/2022









































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









