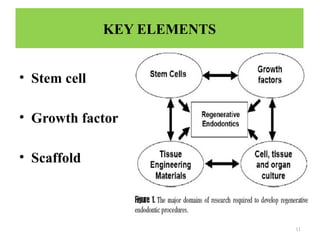
The document discusses regenerative endodontics, emphasizing the potential for using stem cells, growth factors, and scaffolds to regenerate damaged dental pulp and associated structures. It outlines objectives, key elements, methodologies, and technologies involved in the development of regenerative treatments while highlighting the importance of cell sourcing, particularly autologous stem cells. The document also reviews various scaffold materials and their properties, and presents a protocol for revascularization procedures in clinical practice.

























































![the diseases of pulp [Autosaved].pptx for dental students](https://cdn.slidesharecdn.com/ss_thumbnails/thediseasesofpulpautosaved-250422011241-07dc6a61-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














