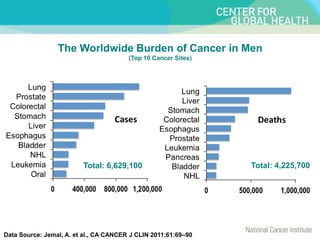
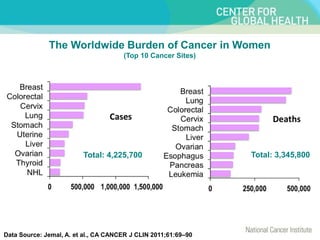
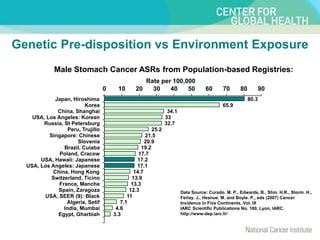
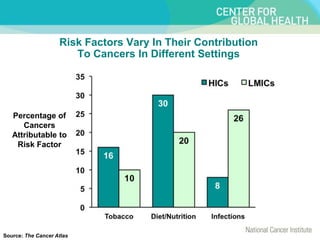
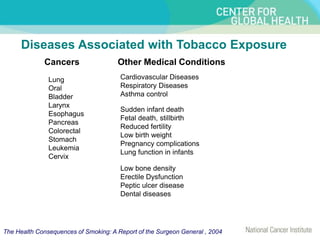
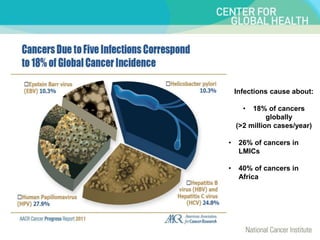
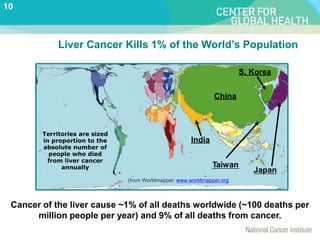
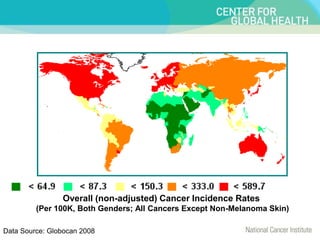
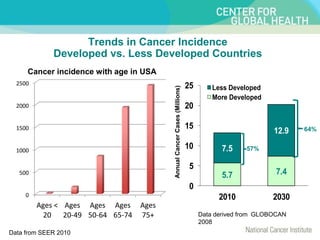
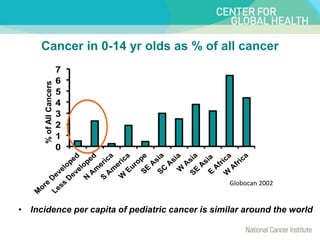
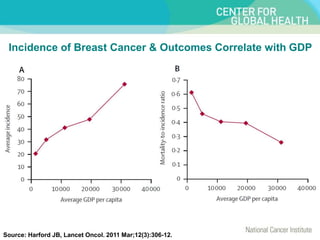
Global cancer rates, types, and mortality vary widely. Eight lifestyle and environmental risk factors account for about 50% of cancer deaths worldwide, with tobacco use being the most significant. While cancer poses tremendous challenges, strategies to reduce risk factors could greatly lower the global cancer burden. Socioeconomic factors also strongly influence cancer rates and outcomes, and this impact is expected to increase in developing countries in the future.