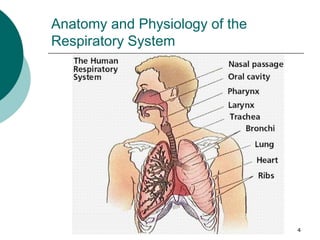
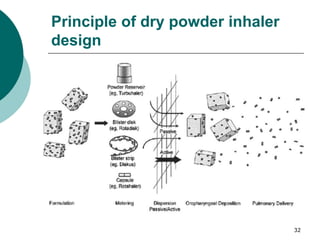
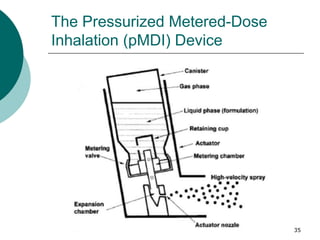
This document discusses pulmonary drug delivery. It begins with the anatomy and physiology of the respiratory system, describing the upper and lower respiratory tracts. It then covers the advantages of pulmonary drug delivery for treating both respiratory and systemic diseases, such as delivering high drug concentrations directly to the disease site while minimizing systemic side effects. The document discusses the different lung epithelium sites that can absorb drugs and the ability to deliver small hydrophobic drugs, small hydrophilic drugs, and macromolecules systemically through inhalation. Finally, it briefly introduces several pulmonary drug delivery devices, including dry powder inhalers, pressurized metered-dose inhalers, and nebulizers.
![Pulmonary drug delivery system [PDDS]](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarydrugdeliverysystem-160619063517-thumbnail.jpg?width=640&height=640&fit=bounds)









































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




