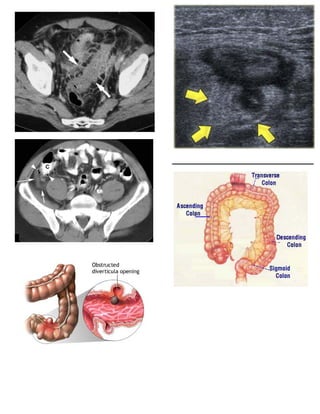
Diverticulitis is inflammation of diverticula in the colon. It can range from mild to severe, with complications including colonic perforation, abscesses, and peritonitis. Symptoms include abdominal pain, fever, and tenderness. Treatment involves antibiotics, clear liquid diets, and sometimes surgery for recurrent or complicated cases.