7th Edition NRPGuidelines
5 year evidence based topic review by
The International Liaison
Committee On Resuscitation.
3.
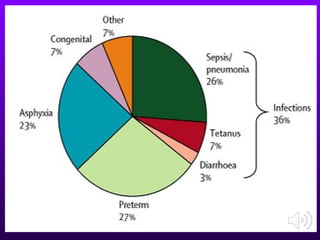
Burden of theproblem
• Birth asphyxia.
• 23% of the causes of neonatal deaths.
• Long term neurological complications.
• Death.
• NNR (Neonatal resuscitation) :simple,
inexpensive, cost effective method.
• Problem: NNR often not initiated, incorrect
use of methods.
5.
2017 NRP MajorChanges
Preparing for resuscitation:
** Team briefing
** Before birth ask:
•What is the suspected gestational age?
•Is the amniotic fluid clear?
•How many babies to expect?
•Are there any additional risk factors?
** Use equipment check lists in pre-
resuscitation briefing .
** In high risk
deliveries equipment should be
unpacked and ready for use.
7.
2017 NRP MajorChanges
Cord Clamping:
• Evidence suggests that cord clamping should be delayed for at least
30 to 60 seconds for most vigorous term and preterm newborns.
• Insufficient evidence for recommendation for infants who require
resuscitation or who have known risk factors for decreased placental
circulation (placental abruption, bleeding placenta previa, bleeding
vasa previa, or cord avulsion(.
Pro: Less IVH, high BPs, higher blood volume,less
need for transfusions and less NEC.
Con: Slightly increased bilirubin levels and need for phototherapy.
Recommendations:
OB will provide delay of cord clamping per request of the patient if the
mother and newborn are clinically stable.
8.
Meconium-stained fluid
Non-vigorous newbornswith meconium-stained fluid do not require
routine intubation and tracheal suctioning; however, meconium-stained
amniotic fluid is a perinatal risk factor that requires presence of one
resuscitation team member with full resuscitation skills, including
endotracheal intubation.
2017 NRP Major Changes
9.
The Golden minute
•The “first minute after birth”
• Anxiety for parents, health providers
• Period of transition from intrauterine to extra
uterine life
• Major: No/minimal assistance
• 10%: assistance to begin breathing at birth
• 1%: extensive resuscitative measures
• First Golden Minute Project: skill based training
10.
Factors for successfulNNR
• Anticipation: call a skilled personnel
• Adequate preparation
• Accurate evaluation, algorithm based
• Prompt initiation of support
12.
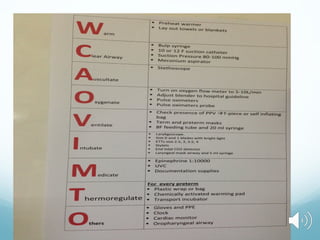
Resuscitation: initial steps
•Provide warmth
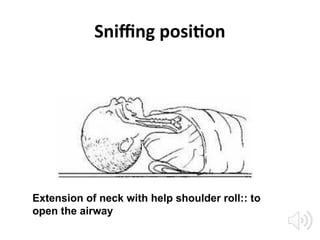
• Head position “ sniffing position”
• Clearing the airway
• Drying the baby
• Tactile stimulation for breathing
Newly born infant
•Specifically the Infant at time of birth
• (A)Do not require resuscitation
• (B)Require resuscitation
• Rapid assessment of 3 characters
– Term gestation?
– Crying or breathing?
– Good muscle tone?
15.
Newly born infant
Termgestation?
Crying or breathing?
Good muscle tone?
YES :Do not require resuscitation
– Dry
– Skin to skin contact
– Covered with dry linen to maintain
temperature
– Ongoing observation: breathing, color, activity
16.
Newly born infant
Termgestation?
Crying or breathing?
Good muscle tone?
NO : require resuscitation; One/more of the
following actions in sequence
– Initial steps in stabilization(warmth, clear
airway, dry, stimulate)
– Ventilation
– Chest compressions
– Administration of epinephrine& /or volume
expansion
< 60 secondsof birth
• If gasping/apnea
If heart rate<100 beats per minute
PPV( positive pressure ventilation)
Spo2 monitoring by pulse oximeter
• Simultaneous evaluation of 3 vitals
• Heart Rate,
• Respiration,
• oxygenation status
21.
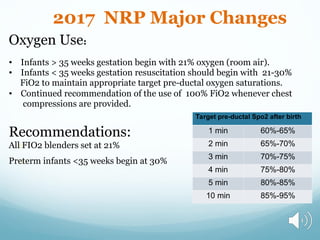
2017 NRP MajorChanges
Oxygen Use:
• Infants > 35 weeks gestation begin with 21% oxygen (room air).
• Infants < 35 weeks gestation resuscitation should begin with 21-30%
FiO2 to maintain appropriate target pre-ductal oxygen saturations.
• Continued recommendation of the use of 100% FiO2 whenever chest
compressions are provided.
Recommendations:
All FIO2 blenders set at 21%
Preterm infants <35 weeks begin at 30%
Target pre-ductal Spo2 after birth
1 min 60%-65%
2 min 65%-70%
3 min 70%-75%
4 min 75%-80%
5 min 80%-85%
10 min 85%-95%
Increase in heartrate is the most
sensitive indicator of a successful
response to each step practiced
24.
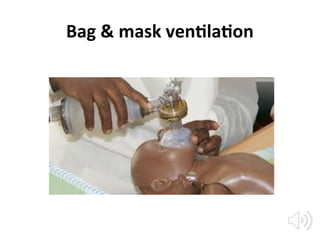
PPV: Positive PressureVentilation
• Form of assisted ventilation
• Needed when there is no improvement in HR
• Also assess chest wall movements
• Should be delivered at rate of 40-60
breaths /min, maintain HR>100 /min
• Devices: BMV, ET (endotracheal
tube),LMA(laryngeal mask airway)
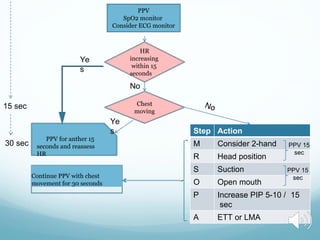
Chest
moving
HR
increasing
within 15
seconds
No
PPV foranther 15
seconds and reassess
HR
Step Action
M Consider 2-hand
R Head position
S Suction
O Open mouth
P Increase PIP 5-10 / 15
sec
A ETT or LMA
PPV 15
sec
Ye
s
Ye
s
15 sec
PPV 15
sec
30 sec
PPV
SpO2 monitor
Consider ECG monitor
Continue PPV with chest
movement for 30 seconds
27.
Endotracheal tube
• Initialendotracheal suctioning of non vigorous
meconium stained new-born.
• If BMV is ineffective/prolonged.
• When chest compressions are performed.
28.
2017 NRP MajorChanges
Endotracheal Intubation and Laryngeal Masks:
•Intubation is strongly recommended prior to
beginning chest
compressions.
•If intubation is not successful or not feasible, a laryngeal mask may
be used.
•Newborns greater than 2 kg and greater than 34 weeks’ gestation
require a size 3.5 endotracheal tube.
•The size 4.0 endotracheal tube is no longer listed on the NRP Quick
Equipment Checklist.
•The vocal cord guide on the endotracheal tube is only an
approximation and may not reliably indicate the correct insertion
depth.
•The tip-to-lip measurement, or depth of the endotracheal tube, is
determined by using the “Initial Endotracheal Tube Insertion
Depth” table or by measuring the nasal-tragus length (NTL).
Chest Compressions:
• Chestcompressions are indicated when the heart rate
remains less than 60 beats/min after at least 30 seconds
of PPV that inflates the lungs, as evidenced by chest
movement with ventilation. In most cases, you should have
given at least 30 seconds of ventilation through a properly
inserted endotracheal tube or laryngeal mask
• Intubation is strongly recommended prior to beginning
chest compressions. If intubation is not successful or not
feasible, a laryngeal mask may be used.
• Chest compressions continue for 60 seconds prior to
checking a heart rate.
2017 NRP Major Changes
33.
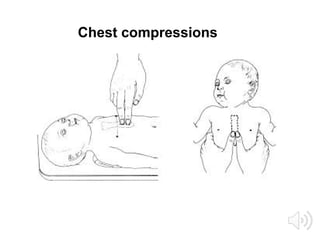
Chest compressions
• Startedwhen HR < 60 per minute despite adequate ventilation
with 100% oxygen for 30 sec
• Delivered at lower third of sternum, to depth 1/3 of AP
diameter of chest
• 2 techniques:
– 2 thumb-encircling hands technique
– Compression with 2 fingers ,second hand supporting the
back
– 3:1 ratio: 90 comp:30 ventilations
– Chest compressions continue for 60 seconds prior to
checking a heart rate.
Volume expansion
• Suspectedor known blood loss
• Isotonic crystalloid solution
• Blood
• Dose calculation: 10 ml/kg
38.
Thermoregulation:
The goal isan axillary temperature between 36.5°C and 37.5°C.
• Increase temperature in the room where the baby will receive initial care to
approximately 23°C to 25°C (74°F–77°F)
• Babies ≥ 33 & ≥1500g: dry with blankets & stimulate
• Babies ≤32 & OR ≤1500g :place wet baby in skin wrap & stimulate
• Apply servo control if remained under wormer for more than a few minutes
• Record axillary & skin temp prior to departure and within 15 minutes of
NICU arrival
2017 NRP Major Changes
39.
Post resuscitation care
•Needed for those who required PPV
• At risk of deterioration
• Need monitoring ,evaluation
• NICU may be necessary
40.
NNR : notindicated
• Conditions with certainly early death
• Extreme prematurity(GA < 24 weeks)
• Birth weight <500g
• Futile conditions such as Anencephaly and
Chromosomal abnormalities: Trisomy 13 and
Trisomy 18
41.
NNR: nearly alwaysindicated
• High rate of survival
• Acceptable morbidity
• GA ≥ 24 weeks
• Those with most congenital malformations
42.
NNR?
• Conditions associatedwith uncertain prognosis
• Survival borderline
• Parental desires concerning initiation of
resuscitation should be supported
43.
Discontinuing resuscitative efforts
•Newly born baby with no detectable heart
rate, consider stopping NNR if the heart rate
remains undetectable for 10 minutes
44.
MCQ1
For successful neonatalresuscitation following
is/are needed except:
1.Anticipation
2.Adequate preparation
3.Skilled personnel
4.Delayed initiation of support
45.
MCQ2
• All thefollowing are true in relation to initial
steps of neonatal resuscitation except
1.Provide warmth
2.Tactile stimulation
3.Clear airway and intubation
4.Drying the baby
46.
MCQ3
• The followingis the primary measure of
adequate ventilation
1.Chest wall movement
2.Improvement in heart rate
3.Pink extremities
4.Spo2 of 80%
47.
MCQ4
• Endotracheal intubationmay be indicated at
several points during neonatal resuscitation
except
1. If BMV is ineffective
2. When chest compressions are performed
3. Endotracheal suctioning of vigorous meconium stained
newborns
4. For special resuscitation circumstances like extremely
LBW
48.
MCQ5
• The recommendedcompression to
ventilation ratio in neonatal resuscitation is
1.2:1
2.3:1
3.4:1
4.5:1
49.
MCQ6
• The recommendeddose(mg/kg per dose) and
route of epinephrine in neonatal resuscitation is
1.0.1-0.3,IV
2.0.01-0.03,IM
3.0.03-0.05,1V
4.0.05-0.1,IV
50.
MCQ7
• Recommended method/clinicalindicator of
confirming ET placement is
1.Condensation in ET
2.Chest movement
3.Equal breath sounds on auscultation
4.Exhaled C02 Detection