Download to read offline



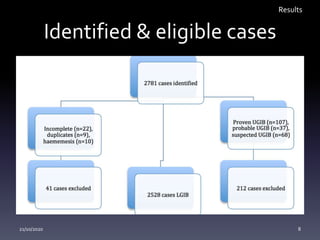
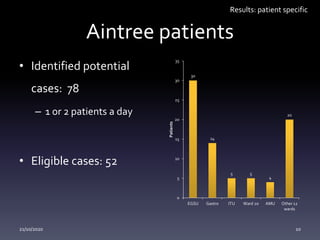
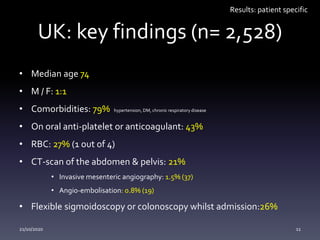
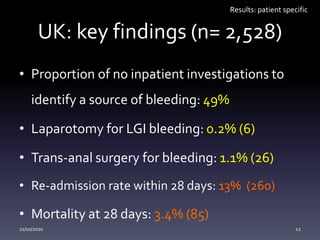

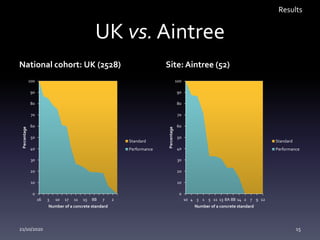
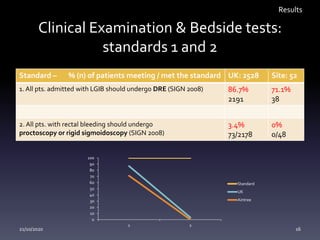
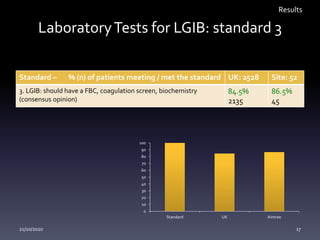
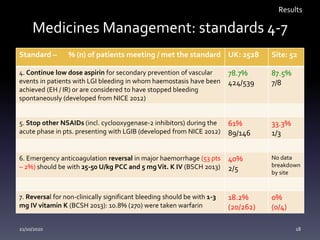
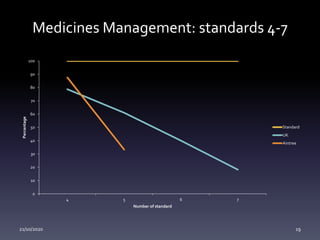
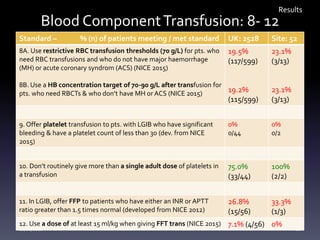
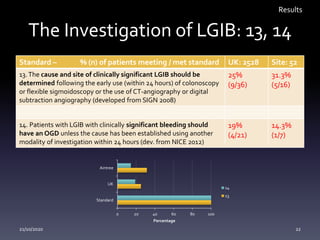
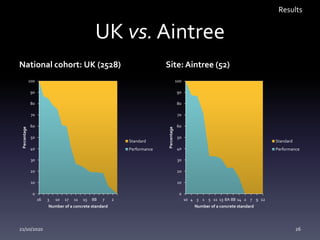


This document summarizes an audit of adult patient characteristics, management, and outcomes related to acute lower gastrointestinal bleeding (LGIB) at hospitals in the UK, including Aintree University Hospital. The audit examined 2,528 patients across 174 UK hospitals and 52 patients at Aintree based on 17 standards of care. Key findings included that 49% of UK patients and 33% of Aintree patients had no inpatient investigations to identify the bleeding source. Performance against the standards was variable both nationally and at Aintree, indicating opportunities for improvement in LGIB management and care.













































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)







