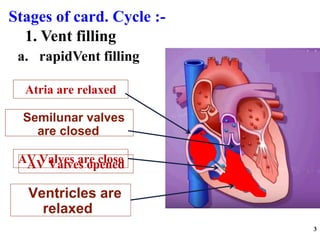
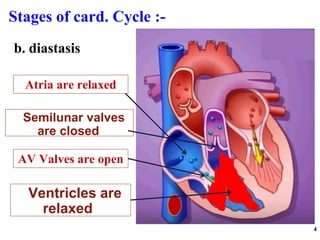
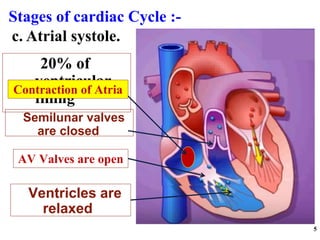
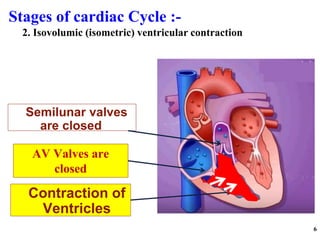
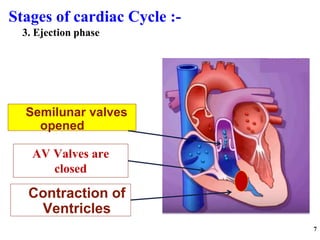
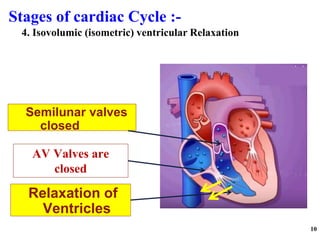
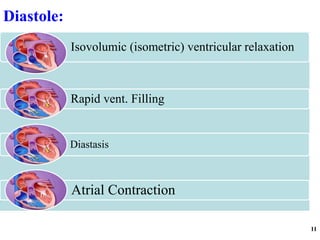
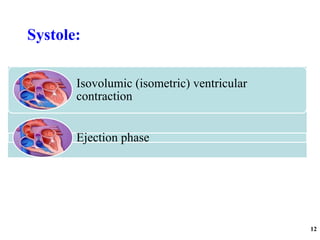
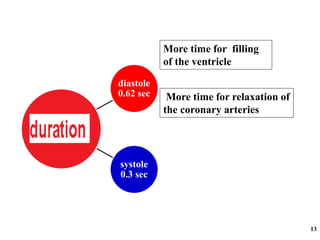
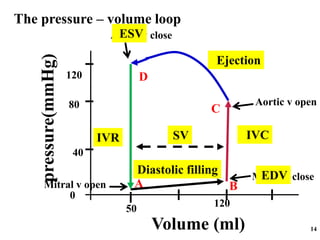
The cardiac cycle has two main phases: diastole and systole. Diastole consists of four stages - ventricular filling, diastasis, atrial systole, and isovolumic ventricular relaxation. Systole consists of isovolumic ventricular contraction, ejection, and isovolumic ventricular relaxation. The cycle aims to relate events like pressure changes, valve movements, and blood flow to electrocardiogram readings and heart sounds over one full heartbeat.