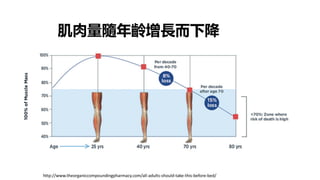
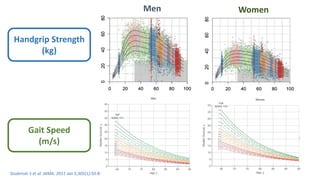
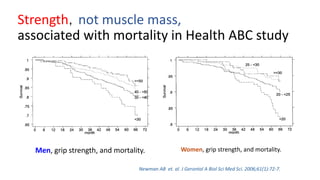
Strength,not muscle mass,
associatedwith mortality in Health ABC study
Newman AB et. al. J Gerontol A Biol Sci Med Sci. 2006;61(1):72-7.
Men, grip strength, and mortality. Women, grip strength, and mortality.
22.
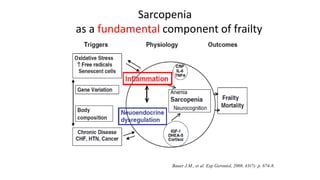
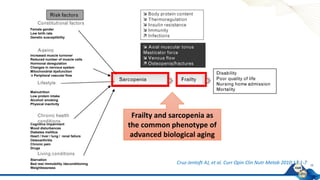
Sarcopenia
ICD-10: M62.84
Age-related progressiveand
generalized skeletal muscle disorder
that involves the accelerated loss of
muscle mass and function
Cruz-Jentoft AJ, Sayer AA. Lancet. 2019;393(10191):2636-2646.
肌少症
22
Acute to chronic
healthcare or
clinical research
sengs
AWGS 2019:
Identifying and diagnosing older adults with or at-risk for sarcopenia
Primary health care
Community preventive services settings
Acute to chronic health care
Clinical research settings
25
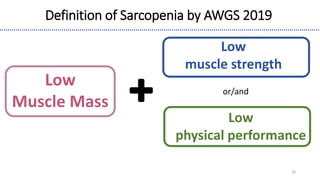
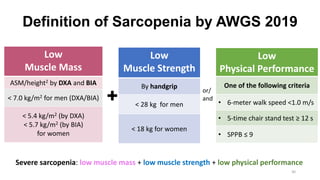
Low
Muscle Mass
ASM/height2 byDXA and BIA
< 7.0 kg/m2 for men (DXA/BIA)
< 5.4 kg/m2 (by DXA)
< 5.7 kg/m2 (by BIA)
for women
Low
Muscle Strength
By handgrip
< 28 kg for men
< 18 kg for women
Low
Physical Performance
One of the following criteria
• 6-meter walk speed <1.0 m/s
• 5-time chair stand test ≥ 12 s
• SPPB ≤ 9
or/
and
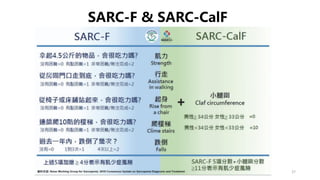
Definition of Sarcopenia by AWGS 2019
Severe sarcopenia: low muscle mass + low muscle strength + low physical performance
30
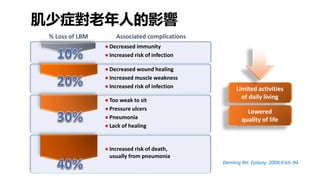
Demling RH. Eplasty.2009;9:65–94
Limited activities
of daily living
Lowered
quality of life
● Decreased immunity
● Increased risk of infection
● Decreased wound healing
● Increased muscle weakness
● Increased risk of infection
● Too weak to sit
● Pressure ulcers
● Pneumonia
● Lack of healing
● Increased risk of death,
usually from pneumonia
% Loss of LBM Associated complications
肌少症對老年人的影響
Sarcopenia and 2-yearrisk of falls in a population of persons aged over 80(N=260 )
25.4% participants diagnosed sarcopenia
Prospective cohort study
(ilSIRENTE Study)
Risk of falling 3X
Landi F et al. Clin Nutr. 2012 Oct;31(5):652-8
肌少症增加跌倒風險
After adjusting for age, gender, cognitive impairment, ADL impairment,
sensory impairments, BMI, depression, physical activity, cholesterol, stroke,
diabetes, number of medications, and C-reactive protein
35.
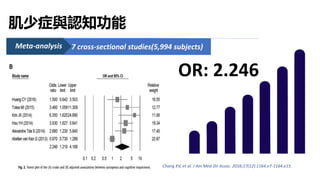
7 cross-sectional studies(5,994subjects)
Meta-analysis
OR: 2.246
Chang KV, et al. J Am Med Dir Assoc. 2016;17(12):1164.e7-1164.e15.
肌少症與認知功能
36.
Yang CP, etal., Aging Cell 2020;19:e13107
肌肉退化影響大腦?
37.
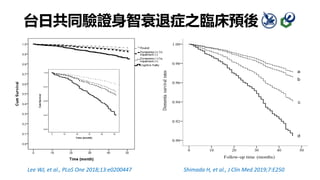
台日共同驗證身智衰退症之臨床預後
Lee WJ, etal., PLoS One 2018;13:e0200447
Follow-up time (months)
Dementia
survival
rates
a
b
c
d
Shimada H, et al., J Clin Med 2019;7:E250
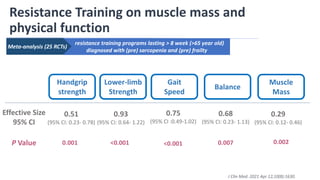
resistance training programslasting > 8 week (>65 year old)
diagnosed with (pre) sarcopenia and (pre) frailty
Resistance Training on muscle mass and
physical function
Handgrip
strength
Lower-limb
Strength
Gait
Speed
Balance
Muscle
Mass
Effective Size
95% CI
0.75
(95% CI :0.49-1.02)
0.29
(95% CI: 0.12- 0.46)
0.68
(95% CI: 0.23- 1.13)
0.93
(95% CI: 0.64- 1.22)
0.51
(95% CI: 0.23- 0.78)
P Value 0.001 <0.001 <0.001 0.002
0.007
Meta-analysis (25 RCTs)
J Clin Med. 2021 Apr 12;10(8):1630.
41.
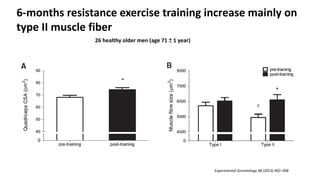
Experimental Gerontology 48(2013) 492–498
6-months resistance exercise training increase mainly on
type II muscle fiber
26 healthy older men (age 71 ± 1 year)
42.
阻力型運動沒有年齡限制
• Increase sizeof both type I and type II muscle fibers
• Improvements in muscle strength and size in healthy older people is similar to
younger people
• Even in very old nursing home residents, resistance exercise training showed
improvements in muscle fiber CSA (3%–9%), muscle strength (> 100%) and physical
performance such as gait speed and stair climbing
42
N Engl J Med. 1994;330:1769–1775
健康老年人跟年輕人透過阻力型運動
進步的肌力與肌肉是相近的
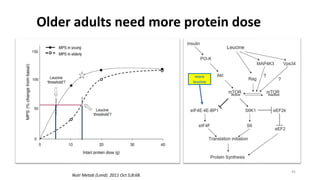
Older adults needmore protein dose
Nutr Metab (Lond). 2011 Oct 5;8:68.
45
more
leucine
46.
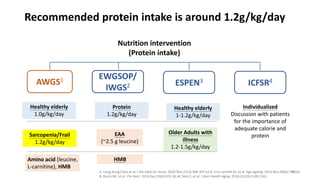
Recommended protein intakeis around 1.2g/kg/day
Nutrition intervention
(Protein intake)
AWGS1 EWGSOP/
IWGS2 ESPEN3 ICFSR4
Protein
1.2g/kg/day
EAA
(~2.5 g leucine)
HMB
Healthy elderly
1.0g/kg/day
Older Adults with
illness
1.2-1.5g/kg/day
Individualized
Discussion with patients
for the importance of
adequate calorie and
protein
1. Liang-Kung Chen et al. J Am Med Dir Assoc. 2020 Mar;21(3):300-307.e2.2. Cruz-Jentoft AJ, et al. Age Ageing. 2014 Nov;43(6):748-59;
3. Deutz NE, et al. Clin Nutr. 2014 Dec;33(6):929-36; 4. Dent E, et al. J Nutr Health Aging. 2018;22(10):1148-1161.
Healthy elderly
1-1.2g/kg/day
Sarcopenia/Frail
1.2g/kg/day
Amino acid (leucine,
L-carnitine), HMB
46
47.
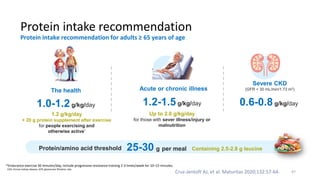
Protein intake recommendation
Cruz-JentoftAJ, et al. Maturitas 2020;132:57-64.
CKD, chronic kidney disease; GFR, glomerular filtration rate.
Protein intake recommendation for adults ≥ 65 years of age
Acute or chronic illness
1.2-1.5g/kg/day
Severe CKD
(GFR < 30 mL/min/1.73 m2)
0.6-0.8 g/kg/day
The health
1.0-1.2g/kg/day
1.2 g/kg/day
+ 20 g protein supplement after exercise
for people exercising and
otherwise active*
Up to 2.0 g/kg/day
for those with sever illness/injury or
malnutrition
*Endurance exercise 30 minutes/day; Include progressive resistance training 2-3 times/week for 10–15 minutes.
Protein/amino acid threshold 25-30 g per meal Containing 2.5-2.8 g leucine
47
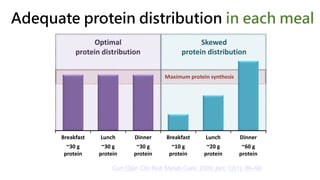
Adequate protein distributionin each meal
Optimal
protein distribution
Skewed
protein distribution
Maximum protein synthesis
Breakfast
~30 g
protein
Lunch
~30 g
protein
Dinner
~30 g
protein
Breakfast
~10 g
protein
Lunch
~20 g
protein
Dinner
~60 g
protein
Curr Opin Clin Nutr Metab Care. 2009 Jan; 12(1): 86–90.
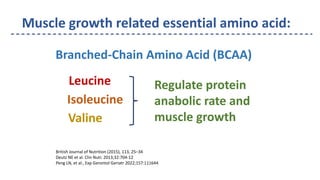
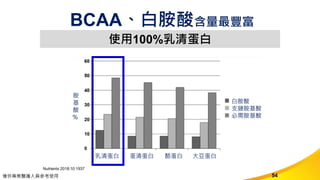
Muscle growth relatedessential amino acid:
Leucine
Isoleucine
Valine
Regulate protein
anabolic rate and
muscle growth
Branched-Chain Amino Acid (BCAA)
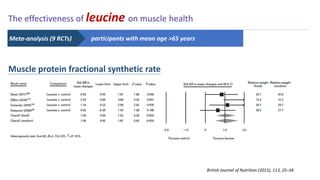
British Journal of Nutrition (2015), 113, 25–34
Deutz NE et al. Clin Nutr. 2013;32:704-12
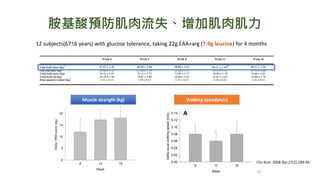
Peng LN, et al., Exp Gerontol Geriatr 2022;157:111644
52.
British Journal ofNutrition (2015), 113, 25–34
The effectiveness of leucine on muscle health
Muscle protein fractional synthetic rate
participants with mean age >65 years
Meta-analysis (9 RCTs)
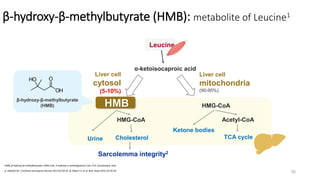
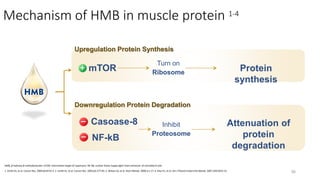
Mechanism of HMBin muscle protein 1-4
1. Smith HJ, et al. Cancer Res. 2004;64:8731-5. 2. Smith HJ, et al. Cancer Res. 2005;65:277-83. 3. Wilson GJ, et al. Nutri Metab. 2008;5:1-17. 4. Eley HL, et al. Am J Physiol Endocrinol Metab. 2007;293:E923-31.
HMB, β-hydroxy-β-methylbutyrate; mTOR, mammalian target of rapamycin; NF-kB, nuclear factor kappa-light-chain-enhancer of activated B cells
56
Upregulation Protein Synthesis
Downregulation Protein Degradation
mTOR
Casoase-8
NF-kB
Turn on
Ribosome Protein
synthesis
Inhibit
Proteosome
Attenuation of
protein
degradation
57.
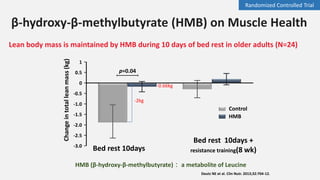
Lean body massis maintained by HMB during 10 days of bed rest in older adults (N=24)
Deutz NE et al. Clin Nutr. 2013;32:704-12.
1
0.5
0
-0.5
-1.0
-1.5
-2.0
-2.5
-3.0
Change
in
total
lean
mass
(kg)
p=0.04
Control
HMB
Bed rest 10days +
resistance training(8 wk)
Bed rest 10days
-2kg
-0.66kg
HMB (β-hydroxy-β-methylbutyrate): a metabolite of Leucine
β-hydroxy-β-methylbutyrate (HMB) on Muscle Health
Randomized Controlled Trial
58.
58
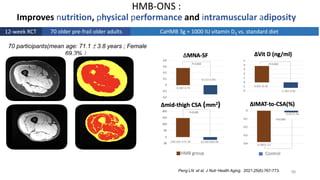
HMB-ONS :
Improves nutrition,physical performance and intramuscular adiposity
Peng LN. et al. J Nutr Health Aging. 2021;25(6):767-773.
70 participants(mean age: 71.1 ± 3.8 years ; Female
69.3%)
12-week RCT CaHMB 3g + 1000 IU vitamin D3 vs. standard diet
70 older pre-frail older adults
59.
59
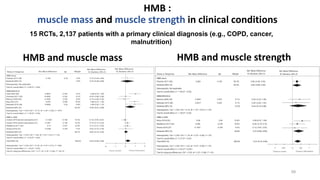
HMB :
muscle massand muscle strength in clinical conditions
Bear DE, et al. Am J Clin Nutr 2019;109:1119-32.
HMB and muscle mass HMB and muscle strength
15 RCTs, 2,137 patients with a primary clinical diagnosis (e.g., COPD, cancer,
malnutrition)
60.
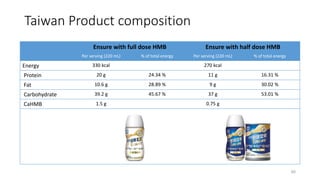
Taiwan Product composition
60
Ensurewith full dose HMB Ensure with half dose HMB
Per serving (220 mL) % of total energy Per serving (220 mL) % of total energy
Energy 330 kcal 270 kcal
Protein 20 g 24.34 % 11 g 16.31 %
Fat 10.6 g 28.89 % 9 g 30.02 %
Carbohydrate 39.2 g 45.67 % 37 g 53.01 %
CaHMB 1.5 g 0.75 g
61.
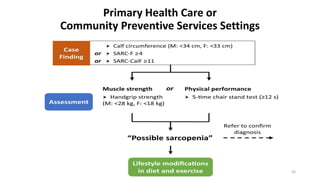
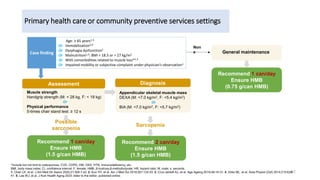
Primary health careor community preventive services settings
61
*Include but not limit to osteoporosis, CVD, COPD, DM, CKD, HTN, immunodeficiency, etc.
BMI, body mass index; CI, confidence interval; F, female; HMB, β-hydroxy-β-methylbutyrate; HR, hazard ratio; M, male; s, seconds.
1. Chen LK, et al. J Am Med Dir Assoc 2020;21:300-7.e2. 2. Kuo YH, et al. Am J Med Sci 2019;357:124-33. 3. Cruz-Jentoft AJ, et al. Age Ageing 2019;48:16-31. 4. Dirks ML, et al. Acta Physiol (Oxf) 2014;210:628-
41. 5. Lee WJ, et al. J Nutr Health Aging 2023; letter to the editor, published online.
Case finding
Age: ≥ 65 years1-3
Or Immobilization3,4
Or Dysphagia dysfunction1
Or Malnutrition1,3: BMI < 18.5 or > 27 kg/m2
Or With comorbidities related to muscle loss*1,3
Or Impaired mobility or subjective complaint under physician’s observation1
Appendicular skeletal muscle mass
DEXA (M: <7.0 kg/m2, F: <5.4 kg/m2)
Or
BIA (M: <7.0 kg/m2, F: <5.7 kg/m2)
Muscle strength
Handgrip strength (M: < 28 kg, F: < 18 kg)
Or
Physical performance
5-times chair stand test: ≥ 12 s
Assessment Diagnosis
Possible
sarcopenia
Sarcopenia
Recommend 1 can/day
Ensure HMB
(1.5 g/can HMB)
Recommend 2 can/day
Ensure HMB
(1.5 g/can HMB)
Non
e General maintenance
Recommend 1 can/day
Ensure HMB
(0.75 g/can HMB)
62.
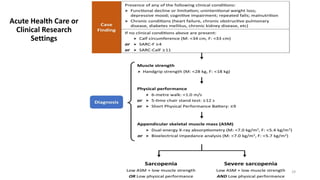
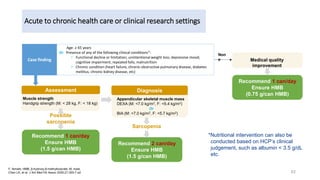
Acute to chronichealth care or clinical research settings
62
F, female; HMB, β-hydroxy-β-methylbutyrate; M, male.
Chen LK, et al. J Am Med Dir Assoc 2020;21:300-7.e2.
Case finding
Age: ≥ 65 years
Or Presence of any of the following clinical conditions*:
• Functional decline or limitation; unintentional weight loss; depressive mood;
cognitive impairment; repeated falls; malnutrition
• Chronic condition (heart failure, chronic obstructive pulmonary disease, diabetes
mellitus, chronic kidney disease, etc)
Muscle strength
Handgrip strength (M: < 28 kg, F: < 18 kg)
Assessment
Possible
sarcopenia
Recommend 1 can/day
Ensure HMB
(1.5 g/can HMB)
Non
e Medical quality
improvement
Recommend 1 can/day
Ensure HMB
(0.75 g/can HMB)
Appendicular skeletal muscle mass
DEXA (M: <7.0 kg/m2, F: <5.4 kg/m2)
Or
BIA (M: <7.0 kg/m2, F: <5.7 kg/m2)
Diagnosis
Sarcopenia
Recommend 2 can/day
Ensure HMB
(1.5 g/can HMB)
*Nutritional intervention can also be
conducted based on HCP’s clinical
judgement, such as albumin < 3.5 g/dL
etc.

































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













