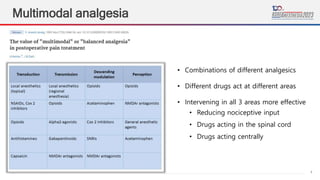
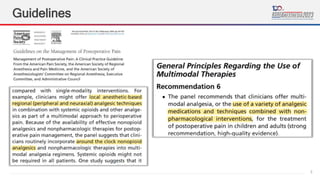
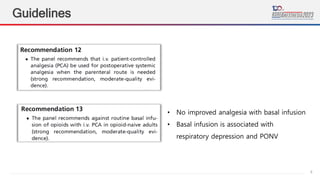
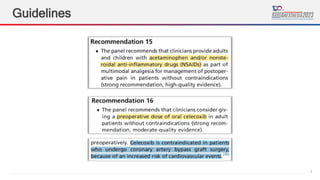
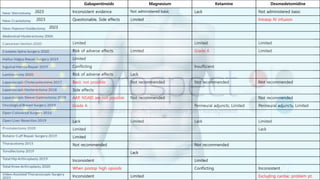
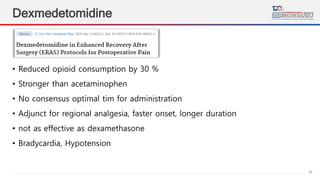
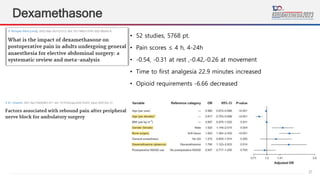
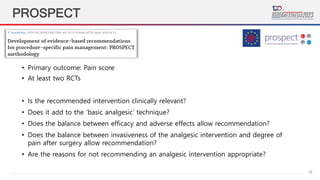
This document provides guidelines and recommendations for perioperative multimodal analgesia. It discusses various analgesic options including paracetamol, NSAIDs, gabapentinoids, ketamine, lidocaine, dexmedetomidine, dexamethasone and regional analgesia techniques. It summarizes guidelines from PROSPECT and other organizations on optimal use of these analgesics alone or in combination to provide effective pain relief with minimal adverse effects in the perioperative period.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




