This document summarizes a pharmacy benefits plan, including coverage details and costs. There is no overall deductible. For generic drugs, the copay is $7 for a 30-day supply. Preferred brand drugs have a $20 copay. Non-preferred brands have a $40 copay. The out-of-pocket maximum is $4,850 single/$7,200 family. Specialty drugs require prior authorization and have a 30% coinsurance. No referral is needed to see a specialist.
Coordination of Benefits and its implications to Health PlansCitiusTech
Coordination of Benefits (COB) allows plans that provide health and/or prescription coverage with Medicare to determine their respective payment responsibilities (i.e. determine which insurance plan has the primary payment responsibility and the extent to which the other plans will contribute when an individual is covered by more than one plan). Member’s primary plan has the responsibility of paying claims first, followed by coverage by remaining plans. This process of splitting the costs across multiple coverage is called COB. This document introduces COB and how health plans and members benefit through COB regulations.
Canadians are often uncertain about the role and limits of their private insurance coverage. Let’s change that.
For this webinar, we were joined by Suzanne Lepage, private health plan specialist, for a discussion of Canada’s private drug plan marketplace and its overlap with government provided services. She walked us through what to expect in terms of coverage and answer audience questions about private insurance. She broke down the Canadian health care system, helped us understand how insurance and employers interact, and gave us tips for contacting our insurance representatives for more information or to appeal the denial of a claim.
She also gave us a tour of the coming changes to Ontario's private insurance marketplace with the introduction of OHIP+.
Coordination of Benefits and its implications to Health PlansCitiusTech
Coordination of Benefits (COB) allows plans that provide health and/or prescription coverage with Medicare to determine their respective payment responsibilities (i.e. determine which insurance plan has the primary payment responsibility and the extent to which the other plans will contribute when an individual is covered by more than one plan). Member’s primary plan has the responsibility of paying claims first, followed by coverage by remaining plans. This process of splitting the costs across multiple coverage is called COB. This document introduces COB and how health plans and members benefit through COB regulations.
Canadians are often uncertain about the role and limits of their private insurance coverage. Let’s change that.
For this webinar, we were joined by Suzanne Lepage, private health plan specialist, for a discussion of Canada’s private drug plan marketplace and its overlap with government provided services. She walked us through what to expect in terms of coverage and answer audience questions about private insurance. She broke down the Canadian health care system, helped us understand how insurance and employers interact, and gave us tips for contacting our insurance representatives for more information or to appeal the denial of a claim.
She also gave us a tour of the coming changes to Ontario's private insurance marketplace with the introduction of OHIP+.
When it comes to health insurance, understanding your options may seem a little daunting. We have put together this presentation to help you understand your options. The first step to choosing the right health insurance for you and your family is understanding your options.
2022 Guide to Improved Patient Outcomes: AI-Powered Remote Monitoring and Inc...Aggregage
A new year means new healthcare challenges. With a soaring need for remote patient monitoring (RPM) as COVID-19 variants spread, 100Plus continues to eliminate patient, clinician, and healthcare system barriers to RPM use. After wide adoption of 100Plus' RPM framework by providers and health care networks, we decided to perform a quality analysis to uncover the impact of our RPM system on key health metrics, and surveyed providers to gather perspectives on how 100Plus' RPM has affected and improved care delivery.
Mintu Turakhia M.D. M.A.S., Director of the Stanford Center for Digital Health and a cardiac electrophysiologist, outcomes researcher, and clinical trialist will present these powerful RPM outcomes.
In this session, you’ll learn:
• How to improve patient outcomes with AI-powered Remote Monitoring Devices
• How you can drive revenue for your practice with RPM CPT codes
• Ways to increase practitioner performance with credible data on patient progression
Healthy Advantage Rewards is a new wellness product offered to employers through Security Health Plan. Visit www.securityhealth.org/healthyrewards for more information.
Medicine the way it used to be.
Ttelemedicine subscription plans allow you to have access to a doctor 24/7 by phone or secure video conference call.
These plans are complimentary to your regular health care plan meaning having a telemedicine plan allows you to speak with a doctor when your regular doctor is not available or it is an emergency and you need to talk to a physician right away.
Think of it as concierge medicine -- access to a doctor when you want for routine health care questions.
The doctors are located in your state and are all board certified.
Telemedicine plans are available for you and your family for $19.95 per month. There is no deductible and no coinsurance.
Telemedicine subscriptions are available to companies. The fee is $10.00 per employee if paid by the company. The plan is portable and you may take the plan with you if you leave the company.
Secure web portals allow you to keep your personal medical information where you may easily find it. It is available in emergency situations or to show your personal doctor.
Prescriptions cards are part of the plan to receive discounts.
I guarantee that you will find this to be a plan of value to help you when you feel most vulnerable, you are not well and you want to speak to a doctor within minutes and not hours or days.
Our Workplace Wellness PowerPoint addresses the concerns of today's businesses and how WillPowerUSA's Workplace Wellness Programs can reduce health care costs and disability claims, and increase productivity and workplace morale.
When it comes to health insurance, understanding your options may seem a little daunting. We have put together this presentation to help you understand your options. The first step to choosing the right health insurance for you and your family is understanding your options.
2022 Guide to Improved Patient Outcomes: AI-Powered Remote Monitoring and Inc...Aggregage
A new year means new healthcare challenges. With a soaring need for remote patient monitoring (RPM) as COVID-19 variants spread, 100Plus continues to eliminate patient, clinician, and healthcare system barriers to RPM use. After wide adoption of 100Plus' RPM framework by providers and health care networks, we decided to perform a quality analysis to uncover the impact of our RPM system on key health metrics, and surveyed providers to gather perspectives on how 100Plus' RPM has affected and improved care delivery.
Mintu Turakhia M.D. M.A.S., Director of the Stanford Center for Digital Health and a cardiac electrophysiologist, outcomes researcher, and clinical trialist will present these powerful RPM outcomes.
In this session, you’ll learn:
• How to improve patient outcomes with AI-powered Remote Monitoring Devices
• How you can drive revenue for your practice with RPM CPT codes
• Ways to increase practitioner performance with credible data on patient progression
Healthy Advantage Rewards is a new wellness product offered to employers through Security Health Plan. Visit www.securityhealth.org/healthyrewards for more information.
Medicine the way it used to be.
Ttelemedicine subscription plans allow you to have access to a doctor 24/7 by phone or secure video conference call.
These plans are complimentary to your regular health care plan meaning having a telemedicine plan allows you to speak with a doctor when your regular doctor is not available or it is an emergency and you need to talk to a physician right away.
Think of it as concierge medicine -- access to a doctor when you want for routine health care questions.
The doctors are located in your state and are all board certified.
Telemedicine plans are available for you and your family for $19.95 per month. There is no deductible and no coinsurance.
Telemedicine subscriptions are available to companies. The fee is $10.00 per employee if paid by the company. The plan is portable and you may take the plan with you if you leave the company.
Secure web portals allow you to keep your personal medical information where you may easily find it. It is available in emergency situations or to show your personal doctor.
Prescriptions cards are part of the plan to receive discounts.
I guarantee that you will find this to be a plan of value to help you when you feel most vulnerable, you are not well and you want to speak to a doctor within minutes and not hours or days.
Our Workplace Wellness PowerPoint addresses the concerns of today's businesses and how WillPowerUSA's Workplace Wellness Programs can reduce health care costs and disability claims, and increase productivity and workplace morale.
Understand how health insurance actually works and then visit us at www.selectmycoverage.com to compare quotes from all the various carriers and even apply online. Should you need assistance, please contact our office. Thanks for checking us out!
Review this presentation to understand how health insurance actually works and then visit us online at www.selectmycoverage.com to obtain a quote and apply
Epistemic Interaction - tuning interfaces to provide information for AI supportAlan Dix
Paper presented at SYNERGY workshop at AVI 2024, Genoa, Italy. 3rd June 2024
https://alandix.com/academic/papers/synergy2024-epistemic/
As machine learning integrates deeper into human-computer interactions, the concept of epistemic interaction emerges, aiming to refine these interactions to enhance system adaptability. This approach encourages minor, intentional adjustments in user behaviour to enrich the data available for system learning. This paper introduces epistemic interaction within the context of human-system communication, illustrating how deliberate interaction design can improve system understanding and adaptation. Through concrete examples, we demonstrate the potential of epistemic interaction to significantly advance human-computer interaction by leveraging intuitive human communication strategies to inform system design and functionality, offering a novel pathway for enriching user-system engagements.
LF Energy Webinar: Electrical Grid Modelling and Simulation Through PowSyBl -...DanBrown980551
Do you want to learn how to model and simulate an electrical network from scratch in under an hour?
Then welcome to this PowSyBl workshop, hosted by Rte, the French Transmission System Operator (TSO)!
During the webinar, you will discover the PowSyBl ecosystem as well as handle and study an electrical network through an interactive Python notebook.
PowSyBl is an open source project hosted by LF Energy, which offers a comprehensive set of features for electrical grid modelling and simulation. Among other advanced features, PowSyBl provides:
- A fully editable and extendable library for grid component modelling;
- Visualization tools to display your network;
- Grid simulation tools, such as power flows, security analyses (with or without remedial actions) and sensitivity analyses;
The framework is mostly written in Java, with a Python binding so that Python developers can access PowSyBl functionalities as well.
What you will learn during the webinar:
- For beginners: discover PowSyBl's functionalities through a quick general presentation and the notebook, without needing any expert coding skills;
- For advanced developers: master the skills to efficiently apply PowSyBl functionalities to your real-world scenarios.
Elevating Tactical DDD Patterns Through Object CalisthenicsDorra BARTAGUIZ
After immersing yourself in the blue book and its red counterpart, attending DDD-focused conferences, and applying tactical patterns, you're left with a crucial question: How do I ensure my design is effective? Tactical patterns within Domain-Driven Design (DDD) serve as guiding principles for creating clear and manageable domain models. However, achieving success with these patterns requires additional guidance. Interestingly, we've observed that a set of constraints initially designed for training purposes remarkably aligns with effective pattern implementation, offering a more ‘mechanical’ approach. Let's explore together how Object Calisthenics can elevate the design of your tactical DDD patterns, offering concrete help for those venturing into DDD for the first time!
Slack (or Teams) Automation for Bonterra Impact Management (fka Social Soluti...Jeffrey Haguewood
Sidekick Solutions uses Bonterra Impact Management (fka Social Solutions Apricot) and automation solutions to integrate data for business workflows.
We believe integration and automation are essential to user experience and the promise of efficient work through technology. Automation is the critical ingredient to realizing that full vision. We develop integration products and services for Bonterra Case Management software to support the deployment of automations for a variety of use cases.
This video focuses on the notifications, alerts, and approval requests using Slack for Bonterra Impact Management. The solutions covered in this webinar can also be deployed for Microsoft Teams.
Interested in deploying notification automations for Bonterra Impact Management? Contact us at sales@sidekicksolutionsllc.com to discuss next steps.
GraphRAG is All You need? LLM & Knowledge GraphGuy Korland
Guy Korland, CEO and Co-founder of FalkorDB, will review two articles on the integration of language models with knowledge graphs.
1. Unifying Large Language Models and Knowledge Graphs: A Roadmap.
https://arxiv.org/abs/2306.08302
2. Microsoft Research's GraphRAG paper and a review paper on various uses of knowledge graphs:
https://www.microsoft.com/en-us/research/blog/graphrag-unlocking-llm-discovery-on-narrative-private-data/
Builder.ai Founder Sachin Dev Duggal's Strategic Approach to Create an Innova...Ramesh Iyer
In today's fast-changing business world, Companies that adapt and embrace new ideas often need help to keep up with the competition. However, fostering a culture of innovation takes much work. It takes vision, leadership and willingness to take risks in the right proportion. Sachin Dev Duggal, co-founder of Builder.ai, has perfected the art of this balance, creating a company culture where creativity and growth are nurtured at each stage.
DevOps and Testing slides at DASA ConnectKari Kakkonen
My and Rik Marselis slides at 30.5.2024 DASA Connect conference. We discuss about what is testing, then what is agile testing and finally what is Testing in DevOps. Finally we had lovely workshop with the participants trying to find out different ways to think about quality and testing in different parts of the DevOps infinity loop.
UiPath Test Automation using UiPath Test Suite series, part 4DianaGray10
Welcome to UiPath Test Automation using UiPath Test Suite series part 4. In this session, we will cover Test Manager overview along with SAP heatmap.
The UiPath Test Manager overview with SAP heatmap webinar offers a concise yet comprehensive exploration of the role of a Test Manager within SAP environments, coupled with the utilization of heatmaps for effective testing strategies.
Participants will gain insights into the responsibilities, challenges, and best practices associated with test management in SAP projects. Additionally, the webinar delves into the significance of heatmaps as a visual aid for identifying testing priorities, areas of risk, and resource allocation within SAP landscapes. Through this session, attendees can expect to enhance their understanding of test management principles while learning practical approaches to optimize testing processes in SAP environments using heatmap visualization techniques
What will you get from this session?
1. Insights into SAP testing best practices
2. Heatmap utilization for testing
3. Optimization of testing processes
4. Demo
Topics covered:
Execution from the test manager
Orchestrator execution result
Defect reporting
SAP heatmap example with demo
Speaker:
Deepak Rai, Automation Practice Lead, Boundaryless Group and UiPath MVP
Smart TV Buyer Insights Survey 2024 by 91mobiles.pdf91mobiles
91mobiles recently conducted a Smart TV Buyer Insights Survey in which we asked over 3,000 respondents about the TV they own, aspects they look at on a new TV, and their TV buying preferences.
Kubernetes & AI - Beauty and the Beast !?! @KCD Istanbul 2024Tobias Schneck
As AI technology is pushing into IT I was wondering myself, as an “infrastructure container kubernetes guy”, how get this fancy AI technology get managed from an infrastructure operational view? Is it possible to apply our lovely cloud native principals as well? What benefit’s both technologies could bring to each other?
Let me take this questions and provide you a short journey through existing deployment models and use cases for AI software. On practical examples, we discuss what cloud/on-premise strategy we may need for applying it to our own infrastructure to get it to work from an enterprise perspective. I want to give an overview about infrastructure requirements and technologies, what could be beneficial or limiting your AI use cases in an enterprise environment. An interactive Demo will give you some insides, what approaches I got already working for real.
Kubernetes & AI - Beauty and the Beast !?! @KCD Istanbul 2024
1 merged documents
1. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2019 – 09/30/2020
Blue Pacific Management: EnvisionRx Pharmacy Plan
1 of 1
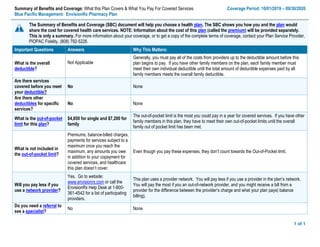
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would
share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, contact your Plan Service Provider,
PIOPAC Fidelity, (808) 792-5226.
Important Questions Answers Why This Matters:
What is the overall
deductible?
Not Applicable
Generally, you must pay all of the costs from providers up to the deductible amount before this
plan begins to pay. If you have other family members on the plan, each family member must
meet their own individual deductible until the total amount of deductible expenses paid by all
family members meets the overall family deductible.
Are there services
covered before you meet
your deductible?
No None
Are there other
deductibles for specific
services?
No None
What is the out-of-pocket
limit for this plan?
$4,850 for single and $7,200 for
family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other
family members in this plan, they have to meet their own out-of-pocket limits until the overall
family out of pocket limit has been met.
What is not included in
the out-of-pocket limit?
Premiums, balance-billed charges,
payments for services subject to a
maximum once you reach the
maximum, any amounts you owe
in addition to your copayment for
covered services, and healthcare
this plan doesn’t cover.
Even though you pay these expenses, they don’t count towards the Out-of-Pocket limit.
Will you pay less if you
use a network provider?
Yes. Go to website:
www.envisionrx.com or call the
EnvisionRx Help Desk at 1-800-
361-4542 for a list of participating
providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.
You will pay the most if you an out-of-network provider, and you might receive a bill from a
provider for the difference between the provider’s charge and what your plan pays) balance
billing).
Do you need a referral to
see a specialist?
No None
2. 2 of 2Questions: 1-808-792-5226
If you are not clear about any of the underlined terms used in this form, call PIOPAC Fidelity, your Plan Service Provider.
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical/Rx Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health
care provider’s office
or clinic
Primary care visit to treat an
injury or illness
Not Applicable Not Applicable
None
Specialist visit Not Applicable Not Applicable None
Preventive care/screening/
immunization
Not Applicable Not Applicable None
If you have a test
Diagnostic test (x-ray, blood
work)
Not Applicable Not Applicable None
Imaging (CT/PET scans, MRIs) Not Applicable Not Applicable None
If you need drugs to
treat your illness or
condition
More information about
prescription drug
coverage is available at
www.envisionrx.com
Generic drugs $7 copay Not Applicable Covers up to a 30-day supply
Preferred brand drugs $20 copay Not Applicable Covers up to a 30-day supply
Non-preferred brand drugs $40 copay Not Applicable Covers up to a 30-day supply
Diabetic Supplies $0 Not Applicable
Applies only to Generic and Preferred Brand
Diabetic Supplies
Specialty drugs 30% Not Applicable
All Specialty drugs are excluded from
coverage including Self- Administered
Injectables (excluding Insulin), fertility agents,
growth Hormones and Hemophilia Factors
EXCEPT FOR THE LISTED MEDICATIONS
LISTED BELOW under Specialty Drugs
covered with Prior Authorization.
Covers up to a 30-day supply
90 Day Retail and
Envision Mail Order
For Maintenance Medication Pay for 2, get 1 Free Not Applicable Covers up to a 90-day supply
Copay Exception
Coinsurance applies if drug
cost is over $150 for 30 DS or
$450 for 90 DS
If the copay is $0.00, the 20%
coinsurance does not apply
20% coinsurance
Not Applicable Formulary Exclusions
Mandatory Generic
Substitution
Preferred Brand or Non-
Preferred Brand Drugs
Brand Name
Copayment will apply
Not Applicable
If a brand name drug is dispensed when a
generic equivalent is available, the brand
3. 3 of 3Questions: 1-808-792-5226
If you are not clear about any of the underlined terms used in this form, call PIOPAC Fidelity, your Plan Service Provider.
Common
Medical/Rx Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
name copayment will Apply PLUS the
difference in cost between the Brand Name
drug and the generic equivalent.
Drug Quantity
Management
Envision Standard
Refer to (If you need
drugs to treat your
illness or condition
Not Applicable
EnvisionRx Standard Formulary is a reference
tool for identifying preferred medication within
certain therapeutic categories
Formulary 2018 Select Formulary
Refer to (If you need
drugs to treat your
illness or condition)
Not Applicable
The drug list (formulary) that is the core of your
prescription drug benefit plan. For complete
formulary drug information visit
www.envisionrx.com
Step Therapy
If you require a medication that
is not on the EnvisionRx
formulary and you cannot use
a formulary alternative, you
have the right to a coverage
determination
Prior-authorization Prior-authorization
PPI, CoxII Inhibitor, Antidepressant, Insomnia
Agents, ADD, Gout, Angiotensin Receptor
Blocker, Cholesterol, Statins, Serotonin and
Norepinephrine Inhibitors, Duexis, Vimovo
Prior Authorization Custom List Not Applicable Not Applicable Formulary Exclusions
Envision Specialty Specialty Drugs 30% Prior Authorization
Specialty Drugs are classified as high cost,
high complexity, specialty drugs are often
injectable or infused
If you have outpatient
surgery
Facility fee (e.g., ambulatory
surgery center)
Not Applicable Not Applicable None
Physician/surgeon fees Not Applicable Not Applicable None
If you need immediate
medical attention
Emergency room care Not Applicable Not Applicable None
Emergency medical
transportation
Not Applicable Not Applicable None
Urgent care Not Applicable Not Applicable None
If you have a hospital
stay
Facility fee (e.g., hospital room) Not Applicable Not Applicable None
Physician/surgeon fees Not Applicable Not Applicable None
4. 4 of 4Questions: 1-808-792-5226
If you are not clear about any of the underlined terms used in this form, call PIOPAC Fidelity, your Plan Service Provider.
Common
Medical/Rx Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you need mental
health, behavioral
health, or substance
abuse services
Outpatient services Not Applicable Not Applicable None
Inpatient services Not Applicable Not Applicable None
If you are pregnant
Office visits Not Applicable Not Applicable None
Childbirth/delivery professional
services
Not Applicable Not Applicable None
Childbirth/delivery facility
services
Not Applicable Not Applicable None
If you need help
recovering or have
other special health
needs
Home health care Not Applicable Not Applicable None
Rehabilitation services Not Applicable Not Applicable None
Habilitation services Not Applicable Not Applicable None
Skilled nursing care Not Applicable Not Applicable None
Durable medical equipment Not Applicable Not Applicable None
Hospice services Not Applicable Not Applicable None
If your child needs
dental or eye care
Children’s eye exam Not Applicable Not Applicable None
Children’s glasses Not Applicable Not Applicable None
Children’s dental check-up Not Applicable Not Applicable None
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those
agencies is: Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more
information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a
grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also
provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance,
contact: Blue Pacific Management Human Resources Department, 808-457-1871 or cwong@bluepacific.com.
Does this plan provide Minimum Essential Coverage? Yes
If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the
requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? Yes
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
7. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Phone 591-0088 • Fax 591-0463 • Toll-Free 800-621-6998 • www.hmaa.com • Customer Service 941-4622 • Toll-Free 888-941-4622
00 ANNU
COMP E-44-2 010119
DEDUCTIBLE
APPLIES
Plan Pays:
Comprehensive Plus
Medical Plan Schedule of Benefits
Annual Deductible $100 per person / $300 maximum per family
Stop Loss $2,000 per person / $6,000 per family (per calendar year, includes deductibles & copayments)
Lifetime Maximum Unlimited
Benefit Coinsurance/Copayment
Participating Non-Participating
Hospital and Facility Services
Ambulatory Surgical Center (ASC) 20% 20%
Hospital Ancillary Services 20% 20%
Hospital Room and Board 20% 20%
Outpatient Facility 20% 20%
Skilled Nursing Facility 20% 20%
Emergency Services
Emergency Room 20% 20%
Physician Visits $15 $15
Online Care and Telephonic Services None Not Covered
Physician Services
Physician Visits $15 $15
Hospital Visits $15 $15
Immunizations (standard, including travel) None None
Testing, Laboratory and Radiology
Allergy Testing 20%* 20%*
Allergy Treatment Materials $5 $5
Diagnostic Testing 20% 20%
Laboratory and Pathology — Inpatient 20% 20%
Outpatient None None
Radiology 20% 20%
Chemotherapy and Radiation Therapy
Chemotherapy — Infusion/Injections 20%* 20%*
Radiation Therapy — Inpatient
Inpatient
20%* 20%*
Outpatient
Inpatient
20% 20%
Other Medical Services and Supplies
Acupuncture, Chiropractic and
Naturopathic Services
20% 20%
Ambulance (air) 20%* 20%*
Ambulance (ground) 20% 20%
Blood and Blood Products 20%* 20%*
Dialysis and Supplies 20%* 20%*
Durable Medical Equipment and Supplies 20%* 20%*
Evaluations for Hearing Aids 20%* 20%*
Growth Hormone Therapy 20% 20%
Home IV Therapy 20% 20%
Inhalation Therapy 20% 20%
Injections 20%* 20%*
Medical Foods 20% 20%
Orthotics and External Prosthetics 20%* 20%*
Vision and Hearing Appliances 20%* 20%*
8. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Note: Reimbursement is based on a percentage of HMAA’s eligible charges, not the billed charges. Eligible charges may be based on a procedure fee
schedule, a percentage of billed charges, per day (per diem) fees, per case fees, per treatment fees, or other methods. This document is intended to
provide a condensed explanation of benefits. Please refer to the Description of Coverage (DOC) for details. In the case of a discrepancy between this
document and the language contained within the DOC, the latter will take precedence.
Benefit Coinsurance/Copayment
Participating Non-Participating
Rehabilitation Therapy
Physical and Occupational Therapy
InpatientInpatient 20% 20%
Outpatient 20%* 20%*
Speech Therapy Services — Inpatient 20% 20%
Outpatient 20%* 20%*
Special Benefits – Disease Management and Preventive Services
Disease Management None Not covered
Preventive Services — Laboratory None None
Preventive Services — Physical Exam None None
Screening and Preventive Counseling None None
Special Benefits for Children
Newborn Care 10% 10%
Well Child Care Immunizations None None
Well Child Care Laboratory Tests None None
Well Child Care Physician Office Visits None None
Special Benefits for Men
Prostate Specific Antigen Test (screening) None None
Special Benefits for Women
Breast Pump None None
Chlamydia Screening None None
Contraceptive Implants (generic) None None
Contraceptive lnjectables (generic) None None
Contraceptive IUD (generic) None None
In Vitro Fertilization 20%* 20%*
Mammography (screening) None None
Maternity Care 10% 10%
Pap Smears (screening) None None
Tubal Ligation None None
Well Woman Exam None None
Special Benefits for Homebound, Terminal, or Long-Term Care
Home Health Care 20% 20%
Hospice Services None None
Behavioral Health – Mental Health and Substance Abuse
Hospital and Facility Services 20% 20%
Physician Services — Inpatient None None
Outpatient $15 $15
Psychological Testing 20% 20%
Special Offers
Employee Assistance Program (EAP) Up to 6 fully-covered visits to assist subscribers with personal or family issues
Health and Wellness Programs A variety of solutions for healthy living including Active&Fit®
, Flu Prevention, Colorectal Cancer
Screening, Maternity & Baby Care Incentive Program, and more
Member Plus Discount Program Discounted prices and special offers from HMAA member groups and other participating
merchants
The Active&Fit and Active&Fit Direct programs are provided by American Specialty Health Fitness, Inc., a subsidiary of American Specialty Health Incorporated
(ASH). Active&Fit Direct, Active&Fit Connected!, Active&Fit, and the Active&Fit Direct logos are trademarks of ASH and used with permission herein.
9. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 01/01/2019
Hawaii Medical Assurance Association: Comprehensive Plus Coverage for: Single/Two-Party/Family | Plan Type: PPO
1 of 6
COMP E-33 010119 (CompPlus)
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the
cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit www.hmaa.com or call 1-888-941-4622.
For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary.
You can view the Glossary at www.hmaa.com or call 1-888-941-4622 to request a copy.
Important Questions Answers Why This Matters:
What is the overall deductible?
$100/Individual or $300/family
Generally, you must pay all of the costs from providers up to the deductible amount before this
plan begins to pay. If you have other family members on the plan, each family member must meet
their own individual deductible until the total amount of deductible expenses paid by all family
members meets the overall family deductible.
Are there services covered
before you meet your
deductible?
Yes. Preventive care, primary care
services, contraceptives, emergency
services, prescription drug and
supplies and well-child care services
are covered before you meet your
deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But
a copayment or coinsurance may apply. For example, this plan covers certain preventive services
without cost-sharing and before you meet your deductible. See a list of covered preventive
services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there other
deductibles for specific
services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit
for this plan?
$2,000/Individual or $6,000/family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other
family members in this plan, they have to meet their own out-of-pocket limits until the overall
family out-of-pocket limit has been met.
What is not included in
the out-of-pocket limit?
Copayments and coinsurance for
certain services, premiums,
balance-billing charges, and health
care this plan doesn’t cover.
Even though you pay these expenses, they do not count toward the out–of–pocket limit.
Will you pay less if you use a
network provider?
Yes. See www.hmaa.com or call
1-888-941-4622 for a list of network
providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.
You will pay the most if you use an out-of-network provider, and you might receive a bill from a
provider for the difference between the provider’s charge and what your plan pays (balance
billing). Be aware, your network provider might use an out-of-network provider for some services
(such as lab work). Check with your provider before you get services.
Do you need a referral to see a
specialist?
No. You can see the specialist you choose without a referral.
OMB Control Numbers 1545‐2229, 1210‐0147, and 0938‐1146
Released on April 6, 2016
10. 2 of 6 COMP E-33 010119 (CompPlus)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health care
provider’s office or clinic
Primary care visit to treat an
injury or illness
$15 copay/office visit;
deductible does not apply
$15 copay/office visit;
deductible does not apply
None
Specialist visit
$15 copay/office visit;
deductible does not apply
$15 copay/office visit;
deductible does not apply
Preventive care/screening/
immunization
No charge No charge
Age and frequency limitations may apply. You
may have to pay for services that aren’t
preventive. Ask your provider if the services
you need are preventive. Then check what
your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood
work)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
NoneNo charge No charge
Imaging (CT/PET scans, MRIs)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
If you need drugs to treat
your illness or condition
More information about
prescription drug
coverage is available at
www.hmaa.com
Generic drugs No charge No charge
Coverage limited to diabetic drugs and
diabetic supplies for all members.
Contraceptives covered for women only.
Only preferred brand named diabetic supplies
are covered at no charge.
Generic diabetic drugs and non-preferred
brand named diabetic drugs and supplies
have a 20% coinsurance.
Diaphragms, cervical caps and generic
contraceptives for women are covered at no
charge when using a network provider.
Preferred brand drugs 20% coinsurance 20% coinsurance
Non-preferred brand drugs 20% coinsurance 20% coinsurance
Specialty drugs No charge No charge
Coverage for specialty drugs limited to oral
chemotherapy only.
If you have outpatient
surgery
Facility fee (e.g., ambulatory
surgery center)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply None
11. 3 of 6 COMP E-33 010119 (CompPlus)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Physician/surgeon fees
$15 copay; deductible
does not apply
$15 copay; deductible does
not apply
If you need immediate
medical attention
Emergency room care
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
None
Emergency medical
transportation
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Coverage for air transportation is limited to the
United States and the deductible applies.
Urgent care
$25 copay; deductible
does not apply
$25 copay; deductible does
not apply
None
If you have a hospital stay
Facility fee (e.g., hospital room)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Physician/surgeon fees
$15 copay; deductible
does not apply
$15 copay; deductible does
not apply
None
If you need mental health,
behavioral health, or
substance abuse services
Outpatient services
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
None
Inpatient services
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
If you are pregnant
Office visits
10% coinsurance;
deductible does not apply
10% coinsurance; deductible
does not apply
None
Childbirth/delivery professional
services
10% coinsurance;
deductible does not apply
10% coinsurance; deductible
does not apply
Childbirth/delivery facility
services
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
If you need help
recovering or have other
special health needs
Home health care
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Coverage limited to 150 days per calendar
year. Preauthorization is required. If you don't
get preauthorization, benefits could be
reduced.
Rehabilitation services
Inpatient: 20%
coinsurance; deductible
does not apply
Inpatient: 20% coinsurance;
deductible does not apply
Preauthorization is required for inpatient
services. If you don't get preauthorization,
benefits could be reduced.Outpatient: 20%
coinsurance
Outpatient: 20% coinsurance
Habilitation services Not covered Not covered None
12. 4 of 6 COMP E-33 010119 (CompPlus)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Skilled nursing care
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Coverage limited to 120 days in any calendar
year.
Durable medical equipment 20% coinsurance 20% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Hospice services No Charge No Charge None
If your child needs dental
or eye care
Children’s eye exam Not covered Not covered None
Children’s glasses Not covered Not covered None
Children’s dental check-up Not covered Not covered None
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
Cosmetic surgery
Dental care (Adult)
Long-term care
Non-emergency care when traveling outside the
U.S.
Private-duty nursing
Routine eye care (Adult)
Routine foot care
Weight loss programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
Acupuncture
Bariatric surgery
Chiropractic care
Hearing aids
Infertility treatment
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is:
HMAA at (888) 941-4622 or CustomerService@hmaa.com, or the Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA (3272) or
www.dol.gov/ebsa/healthreform. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance
Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance
or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete
information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: HMAA at (888) 941-
13. 5 of 6 COMP E-33 010119 (CompPlus)
4622 or CustomerService@hmaa.com, or the Hawaii Insurance Division, ATTN: Health Insurance Branch – External Appeals, 335 Merchant Street, Room 213, Honolulu, HI
96813 at (808) 586-2804 or the Department of Labor Employment Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform.
Does this plan provide Minimum Essential Coverage? Yes.
If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the
requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? Yes.
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
Language Access Services:
Spanish (Español): Para obtener asistencia en Español, llame al 1-888-941-4622.
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-888-941-4622.
Chinese (中文): 如果需要中文的帮助,请拨打这个号码 1-888-941-4622.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-888-941-4622.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
14. 6 of 6 The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby
(9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture
(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes
(a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $100
Specialist copayment $15
Hospital (facility) coinsurance 20%
Other coinsurance 20%
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:
Cost Sharing
Deductibles $0
Copayments $0
Coinsurance $2,000
What isn’t covered
Limits or exclusions $60
The total Peg would pay is $2,060
The plan’s overall deductible $100
Specialist copayment $15
Hospital (facility) coinsurance 20%
Other coinsurance 20%
This EXAMPLE event includes services like:
Primary care physician office visits (including
disease education)
Diagnostic tests (blood work)
Prescription drugs
Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:
Cost Sharing
Deductibles $100
Copayments $150
Coinsurance $1,089
What isn’t covered
Limits or exclusions $55
The total Joe would pay is $1,394
The plan’s overall deductible $100
Specialist copayment $15
Hospital (facility) coinsurance 20%
Other coinsurance 20%
This EXAMPLE event includes services like:
Emergency room care (including medical
supplies)
Diagnostic test (x-ray)
Durable medical equipment (crutches)
Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay:
Cost Sharing
Deductibles $100
Copayments $45
Coinsurance $326
What isn’t covered
Limits or exclusions $0
The total Mia would pay is $471
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be
different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing
amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of
costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
15. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 01/01/2019
Hawaii Medical Assurance Association: Comprehensive Plus Coverage for: Single/Two-Party/Family | Plan Type: PPO
1 of 6
COMP E-33 010119 (CompPlus)
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the
cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit www.hmaa.com or call 1-888-941-4622.
For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary.
You can view the Glossary at www.hmaa.com or call 1-888-941-4622 to request a copy.
Important Questions Answers Why This Matters:
What is the overall deductible?
$100/Individual or $300/family
Generally, you must pay all of the costs from providers up to the deductible amount before this
plan begins to pay. If you have other family members on the plan, each family member must meet
their own individual deductible until the total amount of deductible expenses paid by all family
members meets the overall family deductible.
Are there services covered
before you meet your
deductible?
Yes. Preventive care, primary care
services, contraceptives, emergency
services, prescription drug and
supplies and well-child care services
are covered before you meet your
deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But
a copayment or coinsurance may apply. For example, this plan covers certain preventive services
without cost-sharing and before you meet your deductible. See a list of covered preventive
services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there other
deductibles for specific
services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit
for this plan?
$2,000/Individual or $6,000/family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other
family members in this plan, they have to meet their own out-of-pocket limits until the overall
family out-of-pocket limit has been met.
What is not included in
the out-of-pocket limit?
Copayments and coinsurance for
certain services, premiums,
balance-billing charges, and health
care this plan doesn’t cover.
Even though you pay these expenses, they do not count toward the out–of–pocket limit.
Will you pay less if you use a
network provider?
Yes. See www.hmaa.com or call
1-888-941-4622 for a list of network
providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.
You will pay the most if you use an out-of-network provider, and you might receive a bill from a
provider for the difference between the provider’s charge and what your plan pays (balance
billing). Be aware, your network provider might use an out-of-network provider for some services
(such as lab work). Check with your provider before you get services.
Do you need a referral to see a
specialist?
No. You can see the specialist you choose without a referral.
OMB Control Numbers 1545‐2229, 1210‐0147, and 0938‐1146
Released on April 6, 2016
16. 2 of 6 COMP E-33 010119 (CompPlus)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health care
provider’s office or clinic
Primary care visit to treat an
injury or illness
$15 copay/office visit;
deductible does not apply
$15 copay/office visit;
deductible does not apply
None
Specialist visit
$15 copay/office visit;
deductible does not apply
$15 copay/office visit;
deductible does not apply
Preventive care/screening/
immunization
No charge No charge
Age and frequency limitations may apply. You
may have to pay for services that aren’t
preventive. Ask your provider if the services
you need are preventive. Then check what
your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood
work)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
NoneNo charge No charge
Imaging (CT/PET scans, MRIs)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
If you need drugs to treat
your illness or condition
More information about
prescription drug
coverage is available at
www.hmaa.com
Generic drugs No charge No charge
Coverage limited to diabetic drugs and
diabetic supplies for all members.
Contraceptives covered for women only.
Only preferred brand named diabetic supplies
are covered at no charge.
Generic diabetic drugs and non-preferred
brand named diabetic drugs and supplies
have a 20% coinsurance.
Diaphragms, cervical caps and generic
contraceptives for women are covered at no
charge when using a network provider.
Preferred brand drugs 20% coinsurance 20% coinsurance
Non-preferred brand drugs 20% coinsurance 20% coinsurance
Specialty drugs No charge No charge
Coverage for specialty drugs limited to oral
chemotherapy only.
If you have outpatient
surgery
Facility fee (e.g., ambulatory
surgery center)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply None
17. 3 of 6 COMP E-33 010119 (CompPlus)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Physician/surgeon fees
$15 copay; deductible
does not apply
$15 copay; deductible does
not apply
If you need immediate
medical attention
Emergency room care
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
None
Emergency medical
transportation
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Coverage for air transportation is limited to the
United States and the deductible applies.
Urgent care
$25 copay; deductible
does not apply
$25 copay; deductible does
not apply
None
If you have a hospital stay
Facility fee (e.g., hospital room)
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Physician/surgeon fees
$15 copay; deductible
does not apply
$15 copay; deductible does
not apply
None
If you need mental health,
behavioral health, or
substance abuse services
Outpatient services
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
None
Inpatient services
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
If you are pregnant
Office visits
10% coinsurance;
deductible does not apply
10% coinsurance; deductible
does not apply
None
Childbirth/delivery professional
services
10% coinsurance;
deductible does not apply
10% coinsurance; deductible
does not apply
Childbirth/delivery facility
services
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
If you need help
recovering or have other
special health needs
Home health care
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Coverage limited to 150 days per calendar
year. Preauthorization is required. If you don't
get preauthorization, benefits could be
reduced.
Rehabilitation services
Inpatient: 20%
coinsurance; deductible
does not apply
Inpatient: 20% coinsurance;
deductible does not apply
Preauthorization is required for inpatient
services. If you don't get preauthorization,
benefits could be reduced.Outpatient: 20%
coinsurance
Outpatient: 20% coinsurance
Habilitation services Not covered Not covered None
18. 4 of 6 COMP E-33 010119 (CompPlus)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Skilled nursing care
20% coinsurance;
deductible does not apply
20% coinsurance; deductible
does not apply
Coverage limited to 120 days in any calendar
year.
Durable medical equipment 20% coinsurance 20% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Hospice services No Charge No Charge None
If your child needs dental
or eye care
Children’s eye exam Not covered Not covered None
Children’s glasses Not covered Not covered None
Children’s dental check-up Not covered Not covered None
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
Cosmetic surgery
Dental care (Adult)
Long-term care
Non-emergency care when traveling outside the
U.S.
Private-duty nursing
Routine eye care (Adult)
Routine foot care
Weight loss programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
Acupuncture
Bariatric surgery
Chiropractic care
Hearing aids
Infertility treatment
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is:
HMAA at (888) 941-4622 or CustomerService@hmaa.com, or the Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA (3272) or
www.dol.gov/ebsa/healthreform. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance
Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance
or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete
information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: HMAA at (888) 941-
19. 5 of 6 COMP E-33 010119 (CompPlus)
4622 or CustomerService@hmaa.com, or the Hawaii Insurance Division, ATTN: Health Insurance Branch – External Appeals, 335 Merchant Street, Room 213, Honolulu, HI
96813 at (808) 586-2804 or the Department of Labor Employment Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform.
Does this plan provide Minimum Essential Coverage? Yes.
If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the
requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? Yes.
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
Language Access Services:
Spanish (Español): Para obtener asistencia en Español, llame al 1-888-941-4622.
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-888-941-4622.
Chinese (中文): 如果需要中文的帮助,请拨打这个号码 1-888-941-4622.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-888-941-4622.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
20. 6 of 6 The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby
(9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture
(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes
(a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $100
Specialist copayment $15
Hospital (facility) coinsurance 20%
Other coinsurance 20%
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:
Cost Sharing
Deductibles $0
Copayments $0
Coinsurance $2,000
What isn’t covered
Limits or exclusions $60
The total Peg would pay is $2,060
The plan’s overall deductible $100
Specialist copayment $15
Hospital (facility) coinsurance 20%
Other coinsurance 20%
This EXAMPLE event includes services like:
Primary care physician office visits (including
disease education)
Diagnostic tests (blood work)
Prescription drugs
Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:
Cost Sharing
Deductibles $100
Copayments $150
Coinsurance $1,089
What isn’t covered
Limits or exclusions $55
The total Joe would pay is $1,394
The plan’s overall deductible $100
Specialist copayment $15
Hospital (facility) coinsurance 20%
Other coinsurance 20%
This EXAMPLE event includes services like:
Emergency room care (including medical
supplies)
Diagnostic test (x-ray)
Durable medical equipment (crutches)
Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay:
Cost Sharing
Deductibles $100
Copayments $45
Coinsurance $326
What isn’t covered
Limits or exclusions $0
The total Mia would pay is $471
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be
different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing
amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of
costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
21. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Phone 591-0088 • Fax 591-0463 • Toll-Free 800-621-6998 • www.hmaa.com • Customer Service 941-4622 • Toll-Free 888-941-4622
00 ANNU
COMP E-44-2 010119
DEDUCTIBLE
APPLIES
Plan Pays:
Comprehensive Plus
Medical Plan Schedule of Benefits
Annual Deductible $100 per person / $300 maximum per family
Stop Loss $2,000 per person / $6,000 per family (per calendar year, includes deductibles & copayments)
Lifetime Maximum Unlimited
Benefit Coinsurance/Copayment
Participating Non-Participating
Hospital and Facility Services
Ambulatory Surgical Center (ASC) 20% 20%
Hospital Ancillary Services 20% 20%
Hospital Room and Board 20% 20%
Outpatient Facility 20% 20%
Skilled Nursing Facility 20% 20%
Emergency Services
Emergency Room 20% 20%
Physician Visits $15 $15
Online Care and Telephonic Services None Not Covered
Physician Services
Physician Visits $15 $15
Hospital Visits $15 $15
Immunizations (standard, including travel) None None
Testing, Laboratory and Radiology
Allergy Testing 20%* 20%*
Allergy Treatment Materials $5 $5
Diagnostic Testing 20% 20%
Laboratory and Pathology — Inpatient 20% 20%
Outpatient None None
Radiology 20% 20%
Chemotherapy and Radiation Therapy
Chemotherapy — Infusion/Injections 20%* 20%*
Radiation Therapy — Inpatient
Inpatient
20%* 20%*
Outpatient
Inpatient
20% 20%
Other Medical Services and Supplies
Acupuncture, Chiropractic and
Naturopathic Services
20% 20%
Ambulance (air) 20%* 20%*
Ambulance (ground) 20% 20%
Blood and Blood Products 20%* 20%*
Dialysis and Supplies 20%* 20%*
Durable Medical Equipment and Supplies 20%* 20%*
Evaluations for Hearing Aids 20%* 20%*
Growth Hormone Therapy 20% 20%
Home IV Therapy 20% 20%
Inhalation Therapy 20% 20%
Injections 20%* 20%*
Medical Foods 20% 20%
Orthotics and External Prosthetics 20%* 20%*
Vision and Hearing Appliances 20%* 20%*
22. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Note: Reimbursement is based on a percentage of HMAA’s eligible charges, not the billed charges. Eligible charges may be based on a procedure fee
schedule, a percentage of billed charges, per day (per diem) fees, per case fees, per treatment fees, or other methods. This document is intended to
provide a condensed explanation of benefits. Please refer to the Description of Coverage (DOC) for details. In the case of a discrepancy between this
document and the language contained within the DOC, the latter will take precedence.
Benefit Coinsurance/Copayment
Participating Non-Participating
Rehabilitation Therapy
Physical and Occupational Therapy
InpatientInpatient 20% 20%
Outpatient 20%* 20%*
Speech Therapy Services — Inpatient 20% 20%
Outpatient 20%* 20%*
Special Benefits – Disease Management and Preventive Services
Disease Management None Not covered
Preventive Services — Laboratory None None
Preventive Services — Physical Exam None None
Screening and Preventive Counseling None None
Special Benefits for Children
Newborn Care 10% 10%
Well Child Care Immunizations None None
Well Child Care Laboratory Tests None None
Well Child Care Physician Office Visits None None
Special Benefits for Men
Prostate Specific Antigen Test (screening) None None
Special Benefits for Women
Breast Pump None None
Chlamydia Screening None None
Contraceptive Implants (generic) None None
Contraceptive lnjectables (generic) None None
Contraceptive IUD (generic) None None
In Vitro Fertilization 20%* 20%*
Mammography (screening) None None
Maternity Care 10% 10%
Pap Smears (screening) None None
Tubal Ligation None None
Well Woman Exam None None
Special Benefits for Homebound, Terminal, or Long-Term Care
Home Health Care 20% 20%
Hospice Services None None
Behavioral Health – Mental Health and Substance Abuse
Hospital and Facility Services 20% 20%
Physician Services — Inpatient None None
Outpatient $15 $15
Psychological Testing 20% 20%
Special Offers
Employee Assistance Program (EAP) Up to 6 fully-covered visits to assist subscribers with personal or family issues
Health and Wellness Programs A variety of solutions for healthy living including Active&Fit®
, Flu Prevention, Colorectal Cancer
Screening, Maternity & Baby Care Incentive Program, and more
Member Plus Discount Program Discounted prices and special offers from HMAA member groups and other participating
merchants
The Active&Fit and Active&Fit Direct programs are provided by American Specialty Health Fitness, Inc., a subsidiary of American Specialty Health Incorporated
(ASH). Active&Fit Direct, Active&Fit Connected!, Active&Fit, and the Active&Fit Direct logos are trademarks of ASH and used with permission herein.
23. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Phone 591-0088 • Fax 591-0463 • Toll-Free 800-621-6998 • www.hmaa.com • Customer Service 941-4622 • Toll-Free 888-941-4622
00 ANNU
COMP E-44-1 010119
DEDUCTIBLE
APPLIES
Plan Pays:
Option Plus two
Medical Plan Schedule of Benefits
Annual Deductible $100 per person / $300 maximum per family
Stop Loss $2,500 per person / $7,500 per family (per calendar year, includes deductibles & copayments)
Lifetime Maximum Unlimited
Benefit Coinsurance/Copayment
Participating Non-Participating
Hospital and Facility Services
Ambulatory Surgical Center (ASC) 10% 30%*
Hospital Ancillary Services 10% 30%*
Hospital Room and Board 10% 30%*
Outpatient Facility 10% 30%*
Skilled Nursing Facility 10% 30%*
Emergency Services
Emergency Room 10% 10%
Physician Visits 10% 10%
Online Care and Telephonic Services None Not Covered
Physician Services
Physician Visits 10% 30%*
Hospital Visits 10% 30%*
Immunizations (standard, including travel) None 30%*
Testing, Laboratory and Radiology
Allergy Testing 20%* 30%*
Allergy Treatment Materials 20%* 30%*
Diagnostic Testing — Inpatient 10% 30%*
Outpatient 20% 30%*
Laboratory and Pathology — Inpatient 10% 30%*
Outpatient 20% 30%*
Radiology — Inpatient 10% 30%*
Outpatient 20% 30%*
Chemotherapy and Radiation Therapy
Chemotherapy — Infusion/Injections 20%* 30%*
Radiation Therapy — Inpatient
Inpatient
10% 30%*
Outpatient 20% 30%*
Other Medical Services and Supplies
Acupuncture, Chiropractic, Naturopathic
Services
10% 30%*
Ambulance (air) 20%* 30%*
Ambulance (ground) 20%* 30%*
Blood and Blood Products 20%* 30%*
Dialysis and Supplies 20%* 30%*
Durable Medical Equipment & Supplies 20%* 30%*
Evaluations for Hearing Aids 20% 30%*
Growth Hormone Therapy 20%* 30%*
Home IV Therapy None 30%*
Inhalation Therapy 20%* 30%*
Injections 20%* 30%*
Medical Foods 20% 30%
Orthotics and External Prosthetics 20%* 30%*
Vision and Hearing Appliances 20%* 30%*
24. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Note: Reimbursement is based on a percentage of HMAA’s eligible charges, not the billed charges. Eligible charges may be based on a procedure fee
schedule, a percentage of billed charges, per day (per diem) fees, per case fees, per treatment fees, or other methods. This document is intended to
provide a condensed explanation of benefits. Please refer to the Description of Coverage (DOC) for details. In the case of a discrepancy between this
document and the language contained within the DOC, the latter will take precedence.
Benefit Coinsurance/Copayment
Participating Non-Participating
Rehabilitation Therapy
Physical and Occupational Therapy
InpatientInpatient 10% 30%*
Outpatient 20%* 30%*
Speech Therapy Services — Inpatient 10% 30%*
Outpatient 20%* 30%*
Special Benefits – Disease Management and Preventive Services
Disease Management None Not covered
Preventive Services — Laboratory None 30%*
Preventive Services — Physical Exam None 30%*
Screening and Preventive Counseling None 30%*
Special Benefits for Children
Newborn Care 10% 30%*
Well Child Care Immunizations None None
Well Child Care Laboratory Tests None 30%
Well Child Care Physician Office Visits None 30%
Special Benefits for Men
Prostate Specific Antigen Test (screening) 20% 30%*
Special Benefits for Women
Breast Pump None None*
Chlamydia Screening None 30%*
Contraceptive Implants (generic) None 30%
Contraceptive lnjectables (generic) None 30%
Contraceptive IUD (generic) None 30%
In Vitro Fertilization 10% 30%
Mammography (screening) None 30%
Maternity Care 10% 30%*
Pap Smears (screening) None 30%*
Pregnancy Termination 10% 30%*
Tubal Ligation None 30%*
Well Woman Exam None 30%*
Special Benefits for Homebound, Terminal, or Long-Term Care
Home Health Care None 30%*
Hospice Services None Not covered
Behavioral Health – Mental Health and Substance Abuse
Hospital and Facility Services 10% 30%*
Physician Services 10% 30%*
Psychological Testing — Inpatient 10% 30%*
Outpatient 20% 30%*
Special Offers
Employee Assistance Program (EAP) Up to 6 fully-covered visits to assist subscribers with personal or family issues
Health and Wellness Programs A variety of solutions for healthy living including Active&Fit®
, Flu Prevention, Colorectal Cancer
Screening, Maternity & Baby Care Incentive Program, and more
Member Plus Discount Program Discounted prices and special offers from HMAA member groups and other participating
merchants
The Active&Fit and Active&Fit Direct programs are provided by American Specialty Health Fitness, Inc., a subsidiary of American Specialty Health Incorporated
(ASH). Active&Fit Direct, Active&Fit Connected!, Active&Fit, and the Active&Fit Direct logos are trademarks of ASH and used with permission herein.
25. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 01/01/2019
Hawaii Medical Assurance Association: Option Plus Two Coverage for: Single/Two-Party/Family | Plan Type: PPO
1 of 6
COMP E-31 010119 (OP2)
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the
cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit www.hmaa.com or call 1-888-941-4622.
For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary.
You can view the Glossary at www.hmaa.com or call 1-888-941-4622 to request a copy.
Important Questions Answers Why This Matters:
What is the overall deductible?
$100/Individual or $300/family
Generally, you must pay all of the costs from providers up to the deductible amount before this
plan begins to pay. If you have other family members on the plan, each family member must meet
their own individual deductible until the total amount of deductible expenses paid by all family
members meets the overall family deductible.
Are there services covered
before you meet your
deductible?
Yes. Preventive care, primary care
services, contraceptives, emergency
services, prescription drug and
supplies and well-child care services
are covered before you meet your
deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But
a copayment or coinsurance may apply. For example, this plan covers certain preventive services
without cost-sharing and before you meet your deductible. See a list of covered preventive
services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there other
deductibles for specific
services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit
for this plan?
$2,500/Individual or $7,500/family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other
family members in this plan, they have to meet their own out-of-pocket limits until the overall
family out-of-pocket limit has been met.
What is not included in
the out-of-pocket limit?
Copayments and coinsurance for
certain services, premiums,
balance-billing charges, and health
care this plan doesn’t cover.
Even though you pay these expenses, they do not count toward the out–of–pocket limit.
Will you pay less if you use a
network provider?
Yes. See www.hmaa.com or call
1-888-941-4622 for a list of network
providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.
You will pay the most if you use an out-of-network provider, and you might receive a bill from a
provider for the difference between the provider’s charge and what your plan pays (balance
billing). Be aware, your network provider might use an out-of-network provider for some services
(such as lab work). Check with your provider before you get services.
Do you need a referral to see a
specialist?
No. You can see the specialist you choose without a referral.
OMB Control Numbers 1545‐2229, 1210‐0147, and 0938‐1146
Released on April 6, 2016
26. 2 of 6
COMP E-31 010119 (OP2)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health care
provider’s office or clinic
Primary care visit to treat an
injury or illness
10% coinsurance;
deductible does not apply 30% coinsurance
None
Specialist visit
10% coinsurance;
deductible does not apply 30% coinsurance
Preventive care/screening/
immunization
No charge 30% coinsurance
Age and frequency limitations may apply. You
may have to pay for services that aren’t
preventive. Ask your provider if the services
you need are preventive. Then check what
your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood
work)
20% coinsurance;
deductible does not apply 30% coinsurance
None
Imaging (CT/PET scans, MRIs)
20% coinsurance;
deductible does not apply 30% coinsurance
If you need drugs to treat
your illness or condition
More information about
prescription drug
coverage is available at
www.hmaa.com
Generic drugs No charge 20% coinsurance
Coverage limited to diabetic drugs and
diabetic supplies for all members.
Contraceptives covered for women only.
Only preferred brand named diabetic supplies
are covered at no charge.
Diabetic drugs and non-preferred brand
named diabetic supplies have a 20%
coinsurance. Non-preferred brand named
diabetic drugs have a 30% coinsurance.
Diaphragms, cervical caps and generic
contraceptives for women are covered at no
charge when using a network provider.
Preferred brand drugs 20% coinsurance 20% coinsurance
Non-preferred brand drugs 20% coinsurance 30% coinsurance
Specialty drugs No charge No charge
Coverage for specialty drugs limited to oral
chemotherapy only.
If you have outpatient
surgery
Facility fee (e.g., ambulatory
surgery center)
10% coinsurance;
deductible does not apply
30% coinsurance None
27. 3 of 6
COMP E-31 010119 (OP2)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Physician/surgeon fees
10% coinsurance;
deductible does not apply
30% coinsurance
If you need immediate
medical attention
Emergency room care
10% coinsurance;
deductible does not apply
10% coinsurance; deductible
does not apply
None
Emergency medical
transportation
20% coinsurance 30% coinsurance
Coverage for air transportation is limited to the
United States.
Urgent care
$25 copay; deductible
does not apply
$50 copay; deductible does
not apply
None
If you have a hospital stay
Facility fee (e.g., hospital room)
10% coinsurance;
deductible does not apply
30% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Physician/surgeon fees
10% coinsurance;
deductible does not apply
30% coinsurance
If you need mental health,
behavioral health, or
substance abuse services
Outpatient services
10% coinsurance;
deductible does not apply
30% coinsurance None
Inpatient services
10% coinsurance;
deductible does not apply
30% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
If you are pregnant
Office visits
10% coinsurance;
deductible does not apply
30% coinsurance
None
Childbirth/delivery professional
services
10% coinsurance;
deductible does not apply
30% coinsurance
Childbirth/delivery facility
services
10% coinsurance;
deductible does not apply
30% coinsurance
If you need help
recovering or have other
special health needs
Home health care No charge 30% coinsurance
Coverage limited to 150 days per calendar
year. Preauthorization is required. If you don't
get preauthorization, benefits could be
reduced.
Rehabilitation services
Inpatient: 10%
coinsurance; deductible
does not apply
Inpatient: 30% coinsurance Preauthorization is required for inpatient
services. If you don't get preauthorization,
benefits could be reduced.Outpatient: 20%
coinsurance
Outpatient: 30% coinsurance
28. 4 of 6
COMP E-31 010119 (OP2)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Habilitation services Not covered Not covered None
Skilled nursing care
Inpatient: 10%
coinsurance; deductible
does not apply
30% coinsurance
Coverage limited to 120 days in any calendar
year.
Durable medical equipment 20% coinsurance 30% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Hospice services No Charge Not covered None
If your child needs dental
or eye care
Children’s eye exam Not covered Not covered None
Children’s glasses Not covered Not covered None
Children’s dental check-up Not covered Not covered None
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
Cosmetic surgery
Dental care (Adult)
Long-term care
Non-emergency care when traveling outside the
U.S.
Private-duty nursing
Routine eye care (Adult)
Routine foot care
Weight loss programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
Acupuncture
Bariatric surgery
Chiropractic care
Hearing aids
Infertility treatment
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is:
HMAA at (888) 941-4622 or CustomerService@hmaa.com, or the Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA (3272) or
www.dol.gov/ebsa/healthreform. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance
Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance
or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete
29. 5 of 6
COMP E-31 010119 (OP2)
information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: HMAA at (888) 941-
4622 or CustomerService@hmaa.com, or the Hawaii Insurance Division, ATTN: Health Insurance Branch – External Appeals, 335 Merchant Street, Room 213, Honolulu, HI
96813 at (808) 586-2804 or the Department of Labor Employment Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform.
Does this plan provide Minimum Essential Coverage? Yes.
If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the
requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? Yes.
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
Language Access Services:
Spanish (Español): Para obtener asistencia en Español, llame al 1-888-941-4622.
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-888-941-4622.
Chinese (中文): 如果需要中文的帮助,请拨打这个号码 1-888-941-4622.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-888-941-4622.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
30. 6 of 6 The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby
(9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture
(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes
(a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $100
Specialist coinsurance 10%
Hospital (facility) coinsurance 10%
Other coinsurance 10%
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:
Cost Sharing
Deductibles $0
Copayments $0
Coinsurance $1,364
What isn’t covered
Limits or exclusions $60
The total Peg would pay is $1,424
The plan’s overall deductible $100
Specialist coinsurance 10%
Hospital (facility) coinsurance 10%
Other coinsurance 10%
This EXAMPLE event includes services like:
Primary care physician office visits (including
disease education)
Diagnostic tests (blood work)
Prescription drugs
Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:
Cost Sharing
Deductibles $100
Copayments $0
Coinsurance $1,195
What isn’t covered
Limits or exclusions $55
The total Joe would pay is $1,350
The plan’s overall deductible $100
Specialist coinsurance 10%
Hospital (facility) coinsurance 10%
Other coinsurance 10%
This EXAMPLE event includes services like:
Emergency room care (including medical
supplies)
Diagnostic test (x-ray)
Durable medical equipment (crutches)
Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay:
Cost Sharing
Deductibles $100
Copayments $0
Coinsurance $296
What isn’t covered
Limits or exclusions $0
The total Mia would pay is $396
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be
different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing
amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of
costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
31. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: Beginning on or after 01/01/2019
Hawaii Medical Assurance Association: Option Plus Two Coverage for: Single/Two-Party/Family | Plan Type: PPO
1 of 6
COMP E-31 010119 (OP2)
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the
cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit www.hmaa.com or call 1-888-941-4622.
For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary.
You can view the Glossary at www.hmaa.com or call 1-888-941-4622 to request a copy.
Important Questions Answers Why This Matters:
What is the overall deductible?
$100/Individual or $300/family
Generally, you must pay all of the costs from providers up to the deductible amount before this
plan begins to pay. If you have other family members on the plan, each family member must meet
their own individual deductible until the total amount of deductible expenses paid by all family
members meets the overall family deductible.
Are there services covered
before you meet your
deductible?
Yes. Preventive care, primary care
services, contraceptives, emergency
services, prescription drug and
supplies and well-child care services
are covered before you meet your
deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But
a copayment or coinsurance may apply. For example, this plan covers certain preventive services
without cost-sharing and before you meet your deductible. See a list of covered preventive
services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there other
deductibles for specific
services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit
for this plan?
$2,500/Individual or $7,500/family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other
family members in this plan, they have to meet their own out-of-pocket limits until the overall
family out-of-pocket limit has been met.
What is not included in
the out-of-pocket limit?
Copayments and coinsurance for
certain services, premiums,
balance-billing charges, and health
care this plan doesn’t cover.
Even though you pay these expenses, they do not count toward the out–of–pocket limit.
Will you pay less if you use a
network provider?
Yes. See www.hmaa.com or call
1-888-941-4622 for a list of network
providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.
You will pay the most if you use an out-of-network provider, and you might receive a bill from a
provider for the difference between the provider’s charge and what your plan pays (balance
billing). Be aware, your network provider might use an out-of-network provider for some services
(such as lab work). Check with your provider before you get services.
Do you need a referral to see a
specialist?
No. You can see the specialist you choose without a referral.
OMB Control Numbers 1545‐2229, 1210‐0147, and 0938‐1146
Released on April 6, 2016
32. 2 of 6
COMP E-31 010119 (OP2)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health care
provider’s office or clinic
Primary care visit to treat an
injury or illness
10% coinsurance;
deductible does not apply 30% coinsurance
None
Specialist visit
10% coinsurance;
deductible does not apply 30% coinsurance
Preventive care/screening/
immunization
No charge 30% coinsurance
Age and frequency limitations may apply. You
may have to pay for services that aren’t
preventive. Ask your provider if the services
you need are preventive. Then check what
your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood
work)
20% coinsurance;
deductible does not apply 30% coinsurance
None
Imaging (CT/PET scans, MRIs)
20% coinsurance;
deductible does not apply 30% coinsurance
If you need drugs to treat
your illness or condition
More information about
prescription drug
coverage is available at
www.hmaa.com
Generic drugs No charge 20% coinsurance
Coverage limited to diabetic drugs and
diabetic supplies for all members.
Contraceptives covered for women only.
Only preferred brand named diabetic supplies
are covered at no charge.
Diabetic drugs and non-preferred brand
named diabetic supplies have a 20%
coinsurance. Non-preferred brand named
diabetic drugs have a 30% coinsurance.
Diaphragms, cervical caps and generic
contraceptives for women are covered at no
charge when using a network provider.
Preferred brand drugs 20% coinsurance 20% coinsurance
Non-preferred brand drugs 20% coinsurance 30% coinsurance
Specialty drugs No charge No charge
Coverage for specialty drugs limited to oral
chemotherapy only.
If you have outpatient
surgery
Facility fee (e.g., ambulatory
surgery center)
10% coinsurance;
deductible does not apply
30% coinsurance None
33. 3 of 6
COMP E-31 010119 (OP2)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Physician/surgeon fees
10% coinsurance;
deductible does not apply
30% coinsurance
If you need immediate
medical attention
Emergency room care
10% coinsurance;
deductible does not apply
10% coinsurance; deductible
does not apply
None
Emergency medical
transportation
20% coinsurance 30% coinsurance
Coverage for air transportation is limited to the
United States.
Urgent care
$25 copay; deductible
does not apply
$50 copay; deductible does
not apply
None
If you have a hospital stay
Facility fee (e.g., hospital room)
10% coinsurance;
deductible does not apply
30% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Physician/surgeon fees
10% coinsurance;
deductible does not apply
30% coinsurance
If you need mental health,
behavioral health, or
substance abuse services
Outpatient services
10% coinsurance;
deductible does not apply
30% coinsurance None
Inpatient services
10% coinsurance;
deductible does not apply
30% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
If you are pregnant
Office visits
10% coinsurance;
deductible does not apply
30% coinsurance
None
Childbirth/delivery professional
services
10% coinsurance;
deductible does not apply
30% coinsurance
Childbirth/delivery facility
services
10% coinsurance;
deductible does not apply
30% coinsurance
If you need help
recovering or have other
special health needs
Home health care No charge 30% coinsurance
Coverage limited to 150 days per calendar
year. Preauthorization is required. If you don't
get preauthorization, benefits could be
reduced.
Rehabilitation services
Inpatient: 10%
coinsurance; deductible
does not apply
Inpatient: 30% coinsurance Preauthorization is required for inpatient
services. If you don't get preauthorization,
benefits could be reduced.Outpatient: 20%
coinsurance
Outpatient: 30% coinsurance
34. 4 of 6
COMP E-31 010119 (OP2)
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information
Network Provider
(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Habilitation services Not covered Not covered None
Skilled nursing care
Inpatient: 10%
coinsurance; deductible
does not apply
30% coinsurance
Coverage limited to 120 days in any calendar
year.
Durable medical equipment 20% coinsurance 30% coinsurance
Preauthorization is required. If you don't get
preauthorization, benefits could be reduced.
Hospice services No Charge Not covered None
If your child needs dental
or eye care
Children’s eye exam Not covered Not covered None
Children’s glasses Not covered Not covered None
Children’s dental check-up Not covered Not covered None
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
Cosmetic surgery
Dental care (Adult)
Long-term care
Non-emergency care when traveling outside the
U.S.
Private-duty nursing
Routine eye care (Adult)
Routine foot care
Weight loss programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
Acupuncture
Bariatric surgery
Chiropractic care
Hearing aids
Infertility treatment
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is:
HMAA at (888) 941-4622 or CustomerService@hmaa.com, or the Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA (3272) or
www.dol.gov/ebsa/healthreform. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance
Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance
or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete
35. 5 of 6
COMP E-31 010119 (OP2)
information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: HMAA at (888) 941-
4622 or CustomerService@hmaa.com, or the Hawaii Insurance Division, ATTN: Health Insurance Branch – External Appeals, 335 Merchant Street, Room 213, Honolulu, HI
96813 at (808) 586-2804 or the Department of Labor Employment Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform.
Does this plan provide Minimum Essential Coverage? Yes.
If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the
requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? Yes.
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
Language Access Services:
Spanish (Español): Para obtener asistencia en Español, llame al 1-888-941-4622.
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-888-941-4622.
Chinese (中文): 如果需要中文的帮助,请拨打这个号码 1-888-941-4622.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-888-941-4622.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
36. 6 of 6 The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby
(9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture
(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes
(a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $100
Specialist coinsurance 10%
Hospital (facility) coinsurance 10%
Other coinsurance 10%
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:
Cost Sharing
Deductibles $0
Copayments $0
Coinsurance $1,364
What isn’t covered
Limits or exclusions $60
The total Peg would pay is $1,424
The plan’s overall deductible $100
Specialist coinsurance 10%
Hospital (facility) coinsurance 10%
Other coinsurance 10%
This EXAMPLE event includes services like:
Primary care physician office visits (including
disease education)
Diagnostic tests (blood work)
Prescription drugs
Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:
Cost Sharing
Deductibles $100
Copayments $0
Coinsurance $1,195
What isn’t covered
Limits or exclusions $55
The total Joe would pay is $1,350
The plan’s overall deductible $100
Specialist coinsurance 10%
Hospital (facility) coinsurance 10%
Other coinsurance 10%
This EXAMPLE event includes services like:
Emergency room care (including medical
supplies)
Diagnostic test (x-ray)
Durable medical equipment (crutches)
Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay:
Cost Sharing
Deductibles $100
Copayments $0
Coinsurance $296
What isn’t covered
Limits or exclusions $0
The total Mia would pay is $396
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be
different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing
amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of
costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
37. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Phone 591-0088 • Fax 591-0463 • Toll-Free 800-621-6998 • www.hmaa.com • Customer Service 941-4622 • Toll-Free 888-941-4622
00 ANNU
COMP E-44-1 010119
DEDUCTIBLE
APPLIES
Plan Pays:
Option Plus two
Medical Plan Schedule of Benefits
Annual Deductible $100 per person / $300 maximum per family
Stop Loss $2,500 per person / $7,500 per family (per calendar year, includes deductibles & copayments)
Lifetime Maximum Unlimited
Benefit Coinsurance/Copayment
Participating Non-Participating
Hospital and Facility Services
Ambulatory Surgical Center (ASC) 10% 30%*
Hospital Ancillary Services 10% 30%*
Hospital Room and Board 10% 30%*
Outpatient Facility 10% 30%*
Skilled Nursing Facility 10% 30%*
Emergency Services
Emergency Room 10% 10%
Physician Visits 10% 10%
Online Care and Telephonic Services None Not Covered
Physician Services
Physician Visits 10% 30%*
Hospital Visits 10% 30%*
Immunizations (standard, including travel) None 30%*
Testing, Laboratory and Radiology
Allergy Testing 20%* 30%*
Allergy Treatment Materials 20%* 30%*
Diagnostic Testing — Inpatient 10% 30%*
Outpatient 20% 30%*
Laboratory and Pathology — Inpatient 10% 30%*
Outpatient 20% 30%*
Radiology — Inpatient 10% 30%*
Outpatient 20% 30%*
Chemotherapy and Radiation Therapy
Chemotherapy — Infusion/Injections 20%* 30%*
Radiation Therapy — Inpatient
Inpatient
10% 30%*
Outpatient 20% 30%*
Other Medical Services and Supplies
Acupuncture, Chiropractic, Naturopathic
Services
10% 30%*
Ambulance (air) 20%* 30%*
Ambulance (ground) 20%* 30%*
Blood and Blood Products 20%* 30%*
Dialysis and Supplies 20%* 30%*
Durable Medical Equipment & Supplies 20%* 30%*
Evaluations for Hearing Aids 20% 30%*
Growth Hormone Therapy 20%* 30%*
Home IV Therapy None 30%*
Inhalation Therapy 20%* 30%*
Injections 20%* 30%*
Medical Foods 20% 30%
Orthotics and External Prosthetics 20%* 30%*
Vision and Hearing Appliances 20%* 30%*
38. * = Annual Deductible Applies | % = Coinsurance (Percentage based on eligible charge) | $ = Copayment (Fixed dollar amount)
Note: Reimbursement is based on a percentage of HMAA’s eligible charges, not the billed charges. Eligible charges may be based on a procedure fee
schedule, a percentage of billed charges, per day (per diem) fees, per case fees, per treatment fees, or other methods. This document is intended to
provide a condensed explanation of benefits. Please refer to the Description of Coverage (DOC) for details. In the case of a discrepancy between this
document and the language contained within the DOC, the latter will take precedence.
Benefit Coinsurance/Copayment
Participating Non-Participating
Rehabilitation Therapy
Physical and Occupational Therapy
InpatientInpatient 10% 30%*
Outpatient 20%* 30%*
Speech Therapy Services — Inpatient 10% 30%*
Outpatient 20%* 30%*
Special Benefits – Disease Management and Preventive Services
Disease Management None Not covered
Preventive Services — Laboratory None 30%*
Preventive Services — Physical Exam None 30%*
Screening and Preventive Counseling None 30%*
Special Benefits for Children
Newborn Care 10% 30%*
Well Child Care Immunizations None None
Well Child Care Laboratory Tests None 30%
Well Child Care Physician Office Visits None 30%
Special Benefits for Men
Prostate Specific Antigen Test (screening) 20% 30%*
Special Benefits for Women
Breast Pump None None*
Chlamydia Screening None 30%*
Contraceptive Implants (generic) None 30%
Contraceptive lnjectables (generic) None 30%
Contraceptive IUD (generic) None 30%
In Vitro Fertilization 10% 30%
Mammography (screening) None 30%
Maternity Care 10% 30%*
Pap Smears (screening) None 30%*
Pregnancy Termination 10% 30%*
Tubal Ligation None 30%*
Well Woman Exam None 30%*
Special Benefits for Homebound, Terminal, or Long-Term Care
Home Health Care None 30%*
Hospice Services None Not covered
Behavioral Health – Mental Health and Substance Abuse
Hospital and Facility Services 10% 30%*
Physician Services 10% 30%*
Psychological Testing — Inpatient 10% 30%*
Outpatient 20% 30%*
Special Offers
Employee Assistance Program (EAP) Up to 6 fully-covered visits to assist subscribers with personal or family issues
Health and Wellness Programs A variety of solutions for healthy living including Active&Fit®
, Flu Prevention, Colorectal Cancer
Screening, Maternity & Baby Care Incentive Program, and more
Member Plus Discount Program Discounted prices and special offers from HMAA member groups and other participating
merchants
The Active&Fit and Active&Fit Direct programs are provided by American Specialty Health Fitness, Inc., a subsidiary of American Specialty Health Incorporated
(ASH). Active&Fit Direct, Active&Fit Connected!, Active&Fit, and the Active&Fit Direct logos are trademarks of ASH and used with permission herein.
39. $5,000 Employer paid Life Insurance is included
Comp Basic Bi-Weekly Deduction Comp Plus Bi-Weekly Deduction HMO Bi-Weekly Deduction
Employee Only 1.5% of wages Employee Only $10.46 + 1.5% of wages Employee Only $66.04 + 1.5% of wages
Employee + Spouse $152.57 + 1.5% of wages Employee + Spouse $175.57 + 1.5% of wages Employee + Spouse $292.89 + 1.5% of wages
Employee + Child(ren) $103.99 + 1.5% of wages Employee + Child(ren) $122.82 + 1.5% of wages Employee + Child(ren) $259.91 + 1.5% of wages
Employee + Family $268.5 + 1.5% of wages Employee + Family $300.91 + 1.5% of wages Employee + Family $477.06 + 1.5% of wages
Bi-Weekly Deduction Bi-Weekly Deduction Bi-Weekly Deduction
Employee Only $22.32 + 1.5% of wages Employee Only $32.78 + 1.5% of wages Employee Only $88.36 + 1.5% of wages
Employee + Spouse $199.81 + 1.5% of wages Employee + Spouse $222.81 + 1.5% of wages Employee + Spouse $340.13 + 1.5% of wages
Employee + Child(ren) $149.18 + 1.5% of wages Employee + Child(ren) $168.01 + 1.5% of wages Employee + Child(ren) $305.1 + 1.5% of wages
Employee + Family $339.71 + 1.5% of wages Employee + Family $372.12 + 1.5% of wages Employee + Family $548.27 + 1.5% of wages
Bi-Weekly Deduction Bi-Weekly Deduction Bi-Weekly Deduction
Employee Only 8.57$ Employee Only 12.91$ Employee Only 0.84$
Employee + Spouse 17.14$ Employee + Spouse 28.42$ Employee + Spouse 1.68$
Employee + Child(ren) 18.85$ Employee + Child(ren) 24.54$ Employee + Child(ren) 1.80$
Employee + Family 25.71$ Employee + Family 42.62$ Employee + Family 2.88$
JJC Hawaii, LLC - Jamba Juice Hawaii
MEDICAL BENEFIT PACKAGES AND RATES
Team Member and Team Leader
Effective October 1, 2019 - September 30, 2020
HMAA Comprehensive Plus Plan
VOLUNTARY"Buyup"
HMAA Option Plus Two Plan
VOLUNTARY"Buyup"
Kaiser Permanente
BASEPLAN
Medical Medical Medical
**Default Medical ONLY Plan** HMAA Option Plus Two ONLY Kaiser HMO ONLY
VOLUNTARY"Buyup"
Medical + Drug + Vision + Dental
VOLUNTARY"Buyup"
Medical + Drug + Vision + Dental
VOLUNTARY"Buyup"
VOLUNTARY"StandAlone"
Dental
VOLUNTARY"Add-On"
Pharmacy Add-On
VOLUNTARY"StandAlone"
Dental ONLY *Must be enrolled in a Medical plan Vision ONLY
All bi-weekly deductions (26 pay-periods per year) will be deducted from payroll on a pre-tax basis via the Cafeteria Section 125 Plan, unless you opt-out in writing.
Medical + Drug + Vision + Dental
Package includes HMAA Comp Plus with voluntary Prescription Drug,
Vision and Dental
Package includes HMAA Option Plus Two with voluntary
Prescription Drug, Vision and Dental
Package includes Kaiser Medical with voluntary Prescription
Drug, Vision and Dental
Vision
40. 201
Kaiser Permanente Group Plan 201
Benefit and Payment Chart
3651 BLUE PACIFIC MANAGEMENT
About this chart
This benefit and payment chart:
• Is a summary of covered services and other benefits. It is not a complete description of your benefits. For
coverage criteria, description and limitations of covered Services, and excluded Services, be sure to read
Chapter 1: Important Information, Chapter 3: Benefit Description, and Chapter 4: Services Not Covered.
• Tells you if a covered service or supply is subject to limits or referrals.
• Gives you the page number where you can find the description of your services and other benefits.
• Tells you what your Cost Share is for covered services and supplies.
Note: Special limits may apply to services or other benefits listed in this benefit and payment chart. Please read
the benefit description found on the page referenced by this chart.
You only pay a single Cost Share for covered benefits you receive in the Total Care Service settings. If your care
is not received in a Total Care setting, you pay the Cost Share for each medical service or item in accord with its
relevant benefit section.
Remember, services and other benefits are available only for care you receive when provided, prescribed, or
directed by your KP Hawaii Care Team except for care for Emergency Services and out-of-state Urgent Care.
To find a Medical Office near you visit our website at www.kp.org. For more information on these services see
Chapter 3: Benefit Description. You are encouraged to choose a Personal Care Physician (PCP). You may choose
any PCP that is available to accept you. Parents may choose a pediatrician as the PCP for their child.
You do not need a referral or prior authorization to obstetrical or gynecological care from a health care professional
who specializes in obstetrics or gynecology. Your Physician, however, may have to get prior authorization for
certain Services. Additionally, in accord with state law, you do not need a referral or prior authorization to obtain
access to physical therapy from a physical therapist or Physician who specialized in physical therapy.
Members age 65 and over (excluding Tax Equity and Fiscal Responsibility Act of 1982 ”TEFRA” members) must
meet the required eligibility requirements to receive the benefit of either 1) those listed in this Benefit Summary,
or 2) benefits covered under Original Medicare. See Chapter 9: Coordination of Benefits. Senior Advantage
Members, please refer to your Senior Advantage Evidence of Coverage.
2019 Kaiser Permanente Hawaii’s Guide–GP Page 1 of 8 Benefit Summary
41. Description Cost Share
Annual Copayment Maximum
Member $2,500 per calendar year
Family Unit (3 or more members) $7,500 per calendar year
Annual Deductible
Member None per calendar year
Family Unit None
Routine and Preventive
Health Education and Disease Management
•Physician Visits
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Tobacco Cessation and Counseling Sessions None
•Health education publications None
•Healthy Living Classes Applicable class fees
Immunizations (endorsed by the Centers for Disease
Control and Prevention (CDC))
None
•Office visit for (CDC) Immunizations None
•Office visit for Travel Immunization
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Unexpected Mass Population Immunizations 50% of all Applicable Charges
Office Visits
•Well-Child Care None
•Annual Preventive Care (physical exam) Office Visit None
•Hearing Exam (for correction)
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Vision Exam (for glasses)
•Primary Care $20 per visit
•Specialty Care $20 per visit
Preventive Screenings and Care None
Total Health Assessment (www.kp.org) None
Special Services for Women
Preventive Care
•Annual Gynecological Exam None
•Mammography (screening) None
•Pap Smears (cervical cancer screening) None
Family Planning Visits
•Primary Care $20 per visit
•Specialty Care $20 per visit
Infertility Consultation
•Primary Care $20 per visit
•Specialty Care $20 per visit
In Vitro Fertilization 20% of applicable charges
Maternity
•Maternity Care–routine prenatal visits None
•Maternity Care–delivery 20% of applicable charges
•Maternity Care–one postpartum visit None
2019 Kaiser Permanente Hawaii’s Guide–GP Page 2 of 8 Benefit Summary
42. Description Cost Share
•Maternity and Newborn Length of Stay 20% of applicable charges
•Breast Pump None
Contraceptive Drugs and Devices See Prescription Drugs
Pregnancy Termination
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Total Care Settings Included in Total Care Services
Voluntary Sterilization (including tubal ligation)
•Medical Office •Total Care Settings
Included in Total Care Settings
Special Services for Men
Prostate Specific Antigen (screening) $10 per day
Vasectomy
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Total Care Settings Included in Total Care Settings
Online Care
My Health Manager (www.kp.org) None
Office Visits
Office Visits
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Routine pre-surgical and post-surgical None
Urgent Care Visits
•Within Service Area (Primary Care) $20 per visit
•Within Service Area (Specialty Care) $20 per visit
•Outside Service Area 20% of Applicable Charges
Dependent Child Outside of Service Area
•Routine Primary Care $20 per visit
•Basic laboratory and general imaging $10 per visit
•Testing 20% of applicable charges
•Self-administered drug prescriptions 20% of applicable charges
House Calls
•Primary Care $20 per visit
•Specialty Care $20 per visit
Telehealth $20 per visit; Cost share will vary depending
on service.
2019 Kaiser Permanente Hawaii’s Guide–GP Page 3 of 8 Benefit Summary
43. Description Cost Share
Laboratory, Imaging, and Testing
Laboratory
•Basic $10 per day
•Specialty 20% of applicable charges
Imaging
•Basic $10 per day
•Specialty 20% of applicable charges
Testing
•Allergy Testing
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Skilled-Administered Drugs 20% of applicable charges
•Diagnostic Testing 20% of applicable charges
Surgery
Outpatient Surgery and Procedures
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Total Care Settings Included in Total Care Services
Reconstructive Surgery
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Covered Mastectomy 20% of applicable charges
•Total Care Settings Included in Total Care Services
Total Care Services
You only pay a single Cost Share for covered benefits you receive
in the following Total Care Service settings:
Inpatient Hospital Services 20% of applicable charges
Outpatient Surgery and Procedures in a Hospital-Based Setting
or Ambulatory Surgery Center (ASC)
20% of applicable charges
Emergency Services 20% of applicable charges in area, 20% of
applicable charges out of area.
Observation 20% of applicable charges
Skilled Nursing Facility 20% of applicable charges
Dialysis
•Dialysis 20% applicable charges
•Equipment, Training and Medical Supplies
for home Dialysis
None
Radiation Therapy 20% of applicable charges
Ambulance
Air Ambulance 20% of applicable charges
Ground Ambulance 20% of applicable charges
Physical, Occupational, and Speech Therapy
Physical and Occupational Therapy
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Home Health Care None
•Total Care Settings Included in Total Care Services
Speech Therapy
•Primary Care $20 per visit
2019 Kaiser Permanente Hawaii’s Guide–GP Page 4 of 8 Benefit Summary
44. Description Cost Share
•Specialty Care $20 per visit
•Home Health Care None
•Total Care Settings Included in Total Care Services
Home Health Care and Hospice Care
Home Health Care None
Hospice Care None
Physician Visits
•Primary Care $20 per visit
•Specialty Care $20 per visit
Chemotherapy
•Primary Care $20 per visit
•Specialty Care $20 per visit
•Total Care Settings Included in Total Care Services
Internal, External Prosthetics Devices and Braces
Implanted Internal Prosthetics, Devices and Aids
•Medical Office None
•Total Care Settings Included in Total Care Services
External Prosthetics Devices
•Outpatient 20% of applicable charges
•Total Care Settings Included in Total Care Services
Braces
•Outpatient 20% of applicable charges
•Total Care Settings Included in Total Care Services
Durable Medical equipment
Durable Medical equipment
•Outpatient 20% of applicable charges
•Total Care Settings Included in Total Care Services
Oxygen (for use with DME)
•Outpatient 20% of applicable charges
•Total Care Settings Included in Total Care Services
Repair or Replacement
•Outpatient 20% of applicable charges
•Total Care Settings Included in Total Care Services
Diabetes Equipment 50% of Applicable Charges
Home Phototherapy equipment None
Behavioral Health–Mental Health and Substance
Abuse
Mental Health Care
•Medical Office $20 per visit
•Total Care Settings Included in Total Care Services
Chemical Dependency Care
•Medical Office $20 per visit
2019 Kaiser Permanente Hawaii’s Guide–GP Page 5 of 8 Benefit Summary