
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Femoral Hernia Anatomy, Clinical Features and Surgical Approaches
Similar to Femoral Hernia Anatomy, Clinical Features and Surgical Approaches (20)
More from shahadatsurg
More from shahadatsurg (20)
Recently uploaded
Recently uploaded (20)
Femoral Hernia Anatomy, Clinical Features and Surgical Approaches
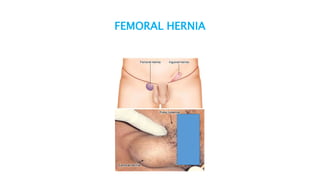
- 2. Diagram
- 3. BASIC ANATOMY OF FEMORAL CANAL 1.25 cm long and 1.25 cm wide. Anteriorly by inguinal ligament. Posteriorly by pelvic bone covered by the iliopectineal ligament (Astley Cooper’s). Medially by lacunar (gimbernat’s) ligament. Laterally by femoral vein.
- 4. CLINICAL FEATURES Common in low weight, elderly women (F>M) More common on right side. Swelling in the groin below and lateral to the pubic tubercle. Impulse on coughing, reducibility, dragging pain. Presents with features of intestinal obstruction— painful, tender, irreducible swelling without any impulse. (50%)
- 5. DIFFERENTIAL DIAGNOSIS 1. Direct inguinal hernia 2. Lymph node 3. Saphena varix 4. Femoral artery aneurysm 5. Psoas abscess 6. Rupture of adductor longus with haematoma
- 6. SURGERY FOR FEMORAL HERNIA
- 7. APPROACHES 1. Low approach (LOCKWOOD) 2. Inguinal approach (LOTHEISSEN) 3. High approach (MCEVEDY) 4. Laparoscopic approach
- 8. VENTRAL HERNIA Any protrusion through abdominal wall with the exception of hernia through the inguinofemoral region is defined as ventral hernia.
- 9. VENTRAL HERNIAS 1. Umbilical–paraumbilical 2. Epigastric 3. Incisional 4. Parastomal 5. Spigelian 6. Lumbar 7. Traumatic
- 10. UMBILICAL HERNIA
- 11. UMBILICAL HERNIAS Umbilical hernia develops due to either absence of umbilical fascia or incomplete closure of umbilical defect. 1. Congenital 2. Acquired Congenital umbilical hernia is common in Africa or in African origin people (8 times).
- 12. FEATURES Occurs in 10% of infants and higher incidence in premature babies Appears within a few weeks of birth Asymptomatic Increases in size on crying Conical shape Both sexes are equally affected
- 13. TREATMENT Conservative under the age of 2 years. 95% will resolve spontaneously. Beyond the age of 2 years surgery is indicated.
- 14. SURGERY
- 15. SURGERY Small curved incision is made immediately below the umbilicus. Neck is opened and contents are returned to the peritoneal cavity. Sac is closed and redundant sac excised. Defect in the linea alba is closed with interrupted sutures.
- 16. EPIGASTRIC HERNIA Midline defect in the linea alba between the xiphoid process and the umbilicus. Occurs at the site where small blood vessels pierce the linea alba. Usually less than 1 cm in maximum diameter and commonly contain only extraperitoneal fat.
- 17. CLINICAL FEATURES Aged between 25 and 40years Soft midline swelling Cough impulse may or may not be felt Can be very painful, due to the partial strangulation Irreducible
- 18. TREATMENT Very small epigastric hernias: disappear spontaneously. Small to- moderate-sized surgery.
- 19. SURGERY Vertical or transverse incision Extraperitoneal fat push back through the defect. Defect is closed with non-absorbable sutures.
- 20. INCISIONAL HERNIA A defect in the musculofascial layers of the abdominal wall in the region of a postoperative scar.
- 21. INCIDENCE 10–50% of laparotomy 1–5% of laparoscopic port-site.
- 22. PREDISPOSING FACTORS Patient factors Obesity Malnutrition Immunosuppression Steroid therapy Chronic cough Cancer
- 23. Wound factors Poor quality tissues Wound infection Vertical incision Layered closure of the abdomen Continuous closure Absorbable suture material has higher chances than non- absorbable sutures
- 24. Surgical factors inappropriate suture material incorrect suture placement Emergency surgery Laparotomy for peritonitis
- 25. CLINICAL FEATURES Localised swelling Skin overlying large hernias; thin and atrophic Peristalsis may be seen Attacks of partial intestinal obstruction
- 26. TREATMENT Principles of surgery a. Repair should cover the whole length of the previous incision. b. Approximation of the musculofascial layers with minimal tension c. Placement of prosthetic mesh.
- 27. SURGERY 1. Open repair 2. Laparoscopic repair
- 28. SPIGELIAN HERNIA • Hernial sac lies either deep to the internal oblique or between external and internal oblique muscles. • It is lateral ventral hernia through Spigelian fascia at any point along its line.
- 29. ANATOMY OF SPIGELIAN HERNIA
- 30. FEATURES Presents as a soft, reducible mass lateral to the rectus muscle and below the umbilicus Impulse on coughing Strangulation can occur Common in females after 50 years
- 31. TREATMENT • Transverse incision herniotomy • Closure of the defect layer by layer using nonabsorbable interrupted sutures.