Spondylolisthesis Diagnosis and Treatment Guide
•
20 likes•1,864 views

The document discusses spondylolisthesis, which refers to the slippage of one vertebra over another. It defines the different types of spondylolisthesis, which include congenital, isthmic, degenerative, traumatic, and pathologic. It also describes the pathophysiology, risk factors, clinical presentation, diagnostic tests, treatment options, and differential diagnosis of spondylolisthesis. The document provides detailed information on spondylolisthesis and aims to educate medical professionals on evaluating and managing this spinal condition.

Recommended
More Related Content
What's hot
What's hot (19)
Viewers also liked
Viewers also liked (20)
Similar to Spondylolisthesis Diagnosis and Treatment Guide
Similar to Spondylolisthesis Diagnosis and Treatment Guide (20)
More from AGRASEN Fracture Arthritis Hospital, Ganesh Nagar,Gondia,Maharashtra,INDIA
More from AGRASEN Fracture Arthritis Hospital, Ganesh Nagar,Gondia,Maharashtra,INDIA (11)
Recently uploaded
Recently uploaded (20)
Spondylolisthesis Diagnosis and Treatment Guide
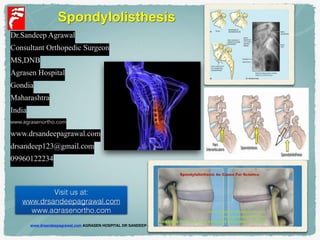
- 1. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Spondylolisthesis Visit us at: www.drsandeepagrawal.com www,agrasenortho.com Dr.Sandeep Agrawal Consultant Orthopedic Surgeon MS,DNB Agrasen Hospital Gondia Maharashtra India www.agrasenortho.com www.drsandeepagrawal.com drsandeep123@gmail.com 09960122234
- 2. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com - OVERVIEW!! - PATHOPHYSIOLOGY & TYPES! - CLINICAL PRESENTATION! - PHYSICAL EXAMINATION! - DIAGNOSIS! - DIAGNOSTIC TESTS! - DIFFERENTIAL DIAGNOSIS! - TREATMENT!! - SUMMARY
- 3. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Spondylolisthesis •Displacement of a cephalad vertebra on the adjacent caudal vertebra •Slipage : anterior, posterior and lateral 3 Spondylolisthesis is derived from the Greek words spondylo , meaning spine, and listhesis , meaning to slip or slide. OVERVIEW (definition) • Lead to a deformity of the spine as well as a narrowing of the spinal canal (central spinal stenosis) or compression of the exiting nerve roots (foraminal stenosis).
- 4. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 4 OVERVIEW ( Anatomy ) Pars interarticulars Spinous process Articular process (inferior) OVERVIEW ( Anatomy)
- 5. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com OVERVIEW (Dermatomes)
- 6. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 6 OVERVIEW (Dermatomes)
- 7. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Classification •Wiltse classification system – anatomy •Meyerding system- by degree of anterior translation
- 8. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 8 It can be classified into 6 distinct categories as the following ( developed by Wiltse, Macnab, and Newman ): TYPES ( according to etiology ) ❑ Type I: Congenital spondylolisthesis ! ❑ Type II: Isthmic spondylolisthesis ! ❑ Type III: Degenerative spondylolisthesis ! ❑ Type IV: Traumatic spondylolisthesis ! ❑ Type V: Pathologic spondylolisthesis ! ❑ Type VI : Postsurgical
- 9. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com • characterized by presence of dysplastic sacral facet joints allowing forward translation of one vertebra relative to another. Type I: Congenital spondylolisthesis ! • Caused by the development of a stress fracture of the pars interarticularis. • It is also further divided into 3 subtypes : Type IIA , type IIB and type IIC . ! Type III: Degenerative spondylolisthesis It is commonly caused by intersegmental instability produced by facet arthropathy. Type II: Isthmic spondylolisthesis
- 10. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type IV: Traumatic spondylolisthesis Caused by fracture or dislocation of the lumbar spine, not involving the pars ! Type VI : Postsurgical (iatrogenic) Type V: Pathologic spondylolisthesis. Caused by malignancy, infection, or other types of abnormal bone
- 11. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com • Heavy Athletic activities requiring predispose some athletes to developing pars defects. ! • Approximately 82% of cases of isthmic spondylolisthesis occur at L5-S1. Another 11.3% occur at L4-L5. ! • Degenerative spondylolisthesis occurs more frequently with increasing age. ! • L4-L5 interspace is affected 6-10 more times than any other level. ! • Sacralization of L5 is frequently seen with L4-5 degenerative spondylolisthesis .
- 12. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com ! ! • Acute isthmic spondylolysis often occurs during the first and second decades of life. Most cases occur before the patient reaches age 15 years. ! • Younger patients are at higher risk than older patients for developing progressive spondylolisthesis. ! • But the risk for progression in adults is rare when the lesion is at L5.. Age
- 13. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type I ( Dysplastic / congenital ) • Failure of formation of the anatomic elements of the lumbosacral facet joint • Axially oriented facet with dyplasia of the superior end plate of the sacrum • Intact pars interarticularis limited splippage < 30% -35 %
- 14. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type II ( Isthmic ) • Presence of a defect in the pars interarticularis ( isthmus ) • Scotty dog sign • Secondary to repetitive microtrauma or a single trauma episode • Subtype A : defect in pars • Subtype B : defect in elongated pars • Subtype C : acute fracture of the pars
- 15. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com • Spondylolisthesis occurs when there’s bilateral defects in the vertebral pars intrarticulariss which permit the vertebral body to slip anteriorly. Usually occurs at level (L5,S1) ! • Spondylolysis is the most common cause for spondylolisthesis. It’s a unilateral or bilateral defect in the vertebral pars interarticularis result from stress fracture. PATHOPHYSIOLOGY
- 16. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type II ( Isthmic ) • Alaskan Eskimos : 26 % • Hyperextension forces
- 17. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type III ( Degenerative ) •Facet joint OA and Hypertrophic lig. flavum
- 18. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 18 ! • spondylolysis typically is acquired as the bone "fatigues" from recurrent microtrauma during excessive lumbar hyperextension or repeated lumbar flexion and extension. • rebeated Hyperflextion and extension of the joints are more common in athletes. • (diving, weight lifting, wrestling and football)
- 19. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com • Spondylolysis progresses to spondylolisthesis in approximately 15% of cases. Progression to spondylolisthesis is correlated with persistent pain and lack of healing.
- 20. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 6- Patients with degenerative spondylolisthesis (DSPL) are characterized by an increased pelvic tilt (PT) and decreased sacral slope (SS) than the control population, suggesting the presence of a pelvic compensation
- 21. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type IV ( Posttraumatic ) •Trauma induce disrupt the posterior arch and its articulations other than pars interarticularis
- 22. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type V ( Pathologic ) •Systemic disease associated : osteogenesis imperfecta, osteopetrosis, arthrogryposis, syphilis •Localized process : infection, neoplasm
- 23. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Type VI ( Postsurgical ) • Laminectomy induced instability • Direct disruption of the facet joint complex • Direct disruption of pars interarticularis • > 50 % posterior facet joint complex removal
- 24. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Meyerding classification • Anterior translation as a percentage of vertebral body on lateral view •Grade I : < 25 % •Grade II : 26-50% •Grade III : 51-75 % •Grade IV : 76 – 100 % •Grade V : > 100 % ( spondyloptosis ) Grade 1 Grade 1 Grade 2 Grade 3 Grade 4 Grade 5 Normal
- 25. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 25 Grades ( Myerding Classification)
- 26. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Presentation and evaluation • Pain at the lumbosacrum junction may radiate to the buttock and posterior thigh but rare below the knee • Restricted motion of lumbar spine • Palpable step-off at L-S junction • Focal kyphosis at L-S junction
- 27. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 1-Phalen-Dickson sign: ! bent-knee, hip-flexed posture with high-grade spondylolisthesis 2-One-legged hyperextension test (stork test): ! Use To differenation between spondylolysis (+) and spondylolisthesis(-) PHYSICAL EXAMINATION
- 28. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com With increasing slippage, the sacrum becomes relatively more vertical, impairing hip extension and compelling the patient to walk with a knee-flexed, hip-flexed gait 1-Phalen-Dickson sign:
- 29. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com A positive one-legged hyperextension test while standing on one leg and bending backward, pain is experienced in the ipsilateral back. 2-One-legged hyperextension test (stork test):
- 30. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com ! ! ! 1- Radiography: lateral view of lumbar spine is especially useful in detection Spondylolisthesis. ! 2- Computed Tomography: CT SCANNING axial or sagittal image of the lumbar spine can be performed with or without contrast enhancment. ! 3- Magnetic Resonance Imaging(MRI): has the distinct advantage of imaging of the spine in any plane. Typically, the axial and sagittal planes are used. ! ! DIAGNOSTEC TESTS
- 31. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com
- 32. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Spondylolisthesis. Oblique projection radiograph shows the presence of bilateral pars defects (arrows), with an appearance resembling a Scottie dog with a collar. (The collar is the pars defect.)
- 33. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com A) -Lateral lumbar spine. Note the pars defects (arrow) and anterior displacement of the L5 vertebra. B) -Oblique lumbar spine. Observe the clearly visible lucent collar (arrow).
- 34. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Sagittal CT reconstruction image shows the pars defect along with grade 1 spondylolisthesis. Spondylolisthesis. Axial CT image shows bilateral spondylolysis (arrows). Note elongation of the spinal canal at this level
- 35. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Image Diagnosis • AP + Lateral L-S views • Stress dynamic view (flexion and extension) - 4 mm Ant. Translation 100 Angulation • Both oblique view for R/O pars fracture
- 36. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com DIFFERENTIAL DIAGNOSIS ! !• Lumber facet-arthropathy . • Coccyx pain. • Mechanical low back pain . • Overuse Injury. • Lumber compression Fracture. • Lumber canal stenosis . • Lumbar disk herniation . ! ! !
- 37. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com • degenerative arthritis affecting the facet joints in the spine • Low back pain can radiate to gluteal, back of the thigh and rarely below the knee. • was no numbness, no muscle weakness and the reflexes were normal. • Stiffness • Poor posture • Radiography: CT and X-ray Lumber facet-arthropathy
- 38. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Axial CT ✓ marked osteophytosis and joint space narrowing ✓ severe osteoarthritis
- 39. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com • Coccydynia is inflammation localized to the tailbone pain and tenderness at coccyx. ! • The pain is often worsened by sitting. • Patient leaning against the buttocks ! • Radiography: CT and X-ray Coccyx pain
- 40. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Lateral radiograph (a) and sagittal CT reconstruction (b) demonstrating a fractured coccyx in a patient who was diagnosed with coccydynia following a ground-level fall 6 months earlier
- 41. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com • fracture of lumber spine due to trauma or pathological fracture in osteomyelitis. • Common in woman who is near or over age 50 . • Sudden back pain radiate to lower limb. numbness and motor weakness in lower limb if nerve roots is affected • Radiography: CT and X-ray Lumber compression Fracture
- 42. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 42 • congenital narrowing of the lumbar spinal canal. • low back pain, • weakness, numbness, pain, and loss of sensation in the legs. • worse pain in standing or walking and backward. It is relieved by sitting and forward. • sphincteric function impairment. • Negative straight leg raising test • Radiography: X-ray, CT and MRI Lumbar canal stenosis
- 43. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Natural history • Multifactorial etiology • 91 % without treatment had lower back pain • 55 % had sciatica • 18 % had neurologic defect • 5 % progression and most in adolescent • Risk factor : slippage > 25% , early disc degeneration
- 44. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com TREATMENT! 1. Conservative . 2. Surgery and Complications 3. Complications !
- 45. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com ➢Treatment for spondylolisthesis depends on several factors, including the age and overall health of the person, the extent of the slip, and the severity of the symptoms. ! ! ➢Treatment most often is conservative and more severe spondylolisthesis might require surgery.
- 46. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Nonsurgical Rx •Mainstay of treatment at < 50 % slippage •Brace : goal to reduce hyperlodosis and stabilize motion •Physiotherapy • Specific training of muscle surrounding the spine
- 47. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 47 ➢Surgery might be necessary if the vertebra continues to slip or if the pain is not relieved by conservative treatment and begins to interfere with daily activities. ! ➢The main goals of surgery for spondylolisthesis are: 1) to relieve the pain associated with an irritated nerve, 2) to stabilize the spine where the vertebra has slipped out of place, 3) and to increase the person’s ability to function. Surgical treatment
- 48. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Surgical Rx •Persistent symptoms (pain and neurologic deficits) affecting quality of life and progression of slip are indicated for surgical Rx. •MRI for further survey (pain source and stenosis )
- 49. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Surgical Rx ! ! • Instrumentation with fusion => better for immediate stability and fusion rate • Low-grade slip with lysis => arthrodesis alone better than decompression + fusion • High-grade slip => fusion in situ with good long term results. • Circumferential fusion (A+P) for good fusion if anterior defect or local kyphosis
- 50. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 2. Fusion ➢ A spinal fusion is normally done immediately after laminectomy for spondylolisthesis. ➢ It is designed to fuse the two vertebrae into one bone and stop the slippage from worsening. ! ➢ The fusion is used to lock the vertebrae in place and stop movement between the vertebrae. ! • Types : A. Traditional Fusion B. Minimally invasive surgical spine fusion
- 51. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 51 A. Traditional Fusion ! ✓ The vertebrae are affixed to one another using surgical instrumentation. ✓ Bone graft is then placed between the vertebrae allowing them to "fuse" together over time. ✓ This stabilizes the painful joint segment and relieves pressure from the painful spinal nerves Examples : 1. Postero-lateral fusion (PLF) 2. Posterior Lumbar Interbody Fusion(PLIF)
- 52. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 1. posterolateral fusion (PLF) ➢ posterolateral fusion is the grandfather of fusion technique as it was developed just over 100 years ago. ➢ In a posterior approach to lumbar fusion, the surgeon makes an incision down the middle of the lower back. ➢ One of the criticisms of PLF is that it involves an extensive dissection (the stripping of muscle and fascia off of bone) of the adjacent transverse processes, facet(s) and sometimes lamina. ➢ After the decompression, the surgeon will place graft material along the sides of the vertebrae to stimulate bone growth. ➢ Titanium screws and rods are often used to provide immediate stability to the spine until a solid fusion has been achieved.
- 53. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com 2. Posterior Lumbar Interbody Fusion(PLIF): ➢ In this procedure, the problem vertebrae are fused from the anterior (front) and posterior (back). ➢ The surgeon works from the back of the spine and removes the disc between the problem vertebrae. ➢ Bone graft material is inserted from the back of the spine into the space between the two vertebrae where the disc was removed (the interbody space) ➢ Transpedicular instrumentation is attached to stabilize the motion segment while fusion occurs.
- 54. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Spondylolytic spondylolisthesis L4,5 L4 Pars fracture
- 55. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Degenerative Spondylolisthsis L4,5 with Spinal Stenosis
- 56. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Degenerative Spondylolisthsis L4,5 with Spinal Stenosis S/P OP
- 57. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com o Implant failure. o Pseudoarthrosis. o Nonunion. o Foot drop. o Spinal compression. o Acute bowel ischaemia Complications of surgical repair
- 58. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com - Spondylolisthesis is a forward or backward slippage of one vertebra on an adjacent vertebra. ! - Causes of spondylolisthesis include trauma, degenerative, tumor, and birth defects. ! - Symptoms of spondylolisthesis include lower back or leg pain, hamstring tightness, and numbness and tingling in the legs. ! - diagnosis is mainly based on imaging . ! - Most people with spondylolisthesis can be treated conservatively, without the need for surgery. ! - Patients who fail to improve with conservative treatment may be a candidate for surgery. SUMMARY
- 59. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Visit us at: www.drsandeepagrawal.com www,agrasenortho.com
- 60. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com This presentation is for doctors in general.! . Some graphics and jpeg files are taken from Google Image to heighten the specific points in this presentation. ! • If there is any objection/or copyright violation, please inform drsandeep123@gmail.com for prompt deletion. ! • It is intended for use only by the doctors of orthopaedic surgery.! . Views expressed in this presentation are personal. • .For any confusion please contact the sole author for clarification. ! • Every body is allowed to copy or download and use the material best suited to him. ! Visit us at:! www.drsandeepagrawal.com! www,agrasenortho.com
- 61. www.drsandeepagrawal.com AGRASEN HOSPITAL DR SANDEEP AGRAWAL GONDIA www.agrasenortho.com Visit us at:! www.drsandeepagrawal.com! www,agrasenortho.com