![Neurocognitive disorder [NCD]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Dementia syndrome
Similar to Dementia syndrome (20)
More from M Ridhwan Abd Razak
More from M Ridhwan Abd Razak (20)
Recently uploaded
Recently uploaded (20)
Dementia syndrome
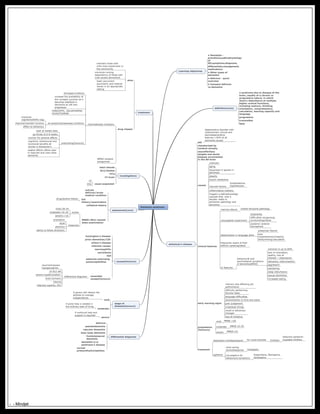
- 1. Dementia syndrome Learning objectives • Dementia - prevalence,pathophysiology of AD,symptoms,diagnosis, differentials,management, medications • Other types of dementia • Delirium - quick overview • Compare delirium vs dementia definition(core) a syndrome due to disease of the brain, usually of a chronic or progressive nature, in which there's disturbance of multiple higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity and language progressive irreversible fatal alzheimer's disease def degenerative disorder with characteristic clinical and deurodegenerative features >50% of all dementia causes charaterised by cerebral atrophy neurofibrillary tangles and senile plaques accumulates in the AD brain causes unknown aging lipoprotein E epsilon 4 genotype obesity insulin resistance vascular factors dyslipidaemia, hypertension inflammatory markers triggers a pathophysiology cascade that, over a decade, leads to alzheimer pathology and dementia clinical features memory failure medial temporal pathology visuospatial impairment dyspraxias difficulties recognising surroundings/faces posterior cerebral hemisphere deterioration in language skills presylvian fissure poor comprehension/reading skills/writing/calculation frequently aware of their deficits-upset/agitated a/ features: behavioural and psychological symptoms of dementia(BPSD) common in up to 60% lack of motivation, apathy, loss of interest-->depression delusions, hallucinations aggression wandering sleep disturbance sexual disinhition increased eating early warning signs memory loss affecting job performance difficulty performing familiar tasks language difficulties disorientation to time and place poor judgement misplaced things mood or behaviour changes loss of initiative progression (honours) mild MMSE >20 moderate MMSE 10-20 severe MMSE<10 treatment depression-antidepressants for mood disorder Subtopic Selective serotonin reuptake inhibitor agitation short acting benzodiazepines lorazepam neuroleptics for behavioura symptoms Risperidane, Olansepine, Quietiapine differential diagnosis delirium pseudodementia vascular dementia lewy body dementia frontotemporal dementia dementia a/w parkinson's disease normal pressurehydrocephalus stage of disease(honours) mild if person still retains the abilities to manage independently moderate if some help is needed in the ordinary task of living severe if continual help and support is required causes(honours) huntington's disease prion dementias/CJD wilson's disease infective causes neurosyphilis sarcoidosis HIV subacute sclerosing panencephalities reversible causes(honours) differential diagnosis recurrent/severe hypoglycaemia vit B12 def severe hypothyroidism brain tumours trauma infection-syphilis, HIV assessment(core) outrule delirium/acute medical condition full history/examination drug/alcohol history collateral history MMSE=Mini–mental state examination scores mild=30-24 moderate=16-20 severe=<16 measures orientation recall attention ability to follow directions investigations basic bloods B12/folates TFTs CT brain cause suspected LP EEG treatment aims maintain those with mild-mod impairment in the community minimise nursing dependency of those with mod-severe dementia# treat concurrent psychiatric and medical issues in an appropriate setting drug classes cholinesterase inhibitors strongest evidence increase the availability of Ach synaptic junction as it becomes depleted in dementia as cell loss progresses DONAZEPIL, GALANTAMINE, RIVASTIGMINE all acetylcholinesterase inhibitors improves cognition(ADAS-cog) improve/maintain function effect on behaviour prescribing(honours) start at lowest dose up titrate at 6-8 weeks monitor for adverse effects cognitive, behavioural and functional benefits all similar in Alzheimer's weaker effects oftens seen in Vascular and Lewy body dementia NMDA receptor antagonists - - Mindjet