Cardiovascular System Problems in GP
•
20 likes•1,566 views

Cardio vascular Problems in GP – By Prof.Dr.R.R.Deshpande • These ppts will be very useful for Medical students & New Practioners ,for rapid revisions of topic & as ready reference through their smart phones .This PPT contains Differential Diagnosis of Acute Chest Pain,Angina Pectoris, Myocardial Infarction, Hypertension, Palpitation, Congestive Cardiac Failure ( CCF) .Causes, Symptoms, Investigations, Modern & Ayurvedic Treatment is given • Visit – www.ayurvedicfriend.com M- 9226810630

Recommended
Recommended
More Related Content
What's hot
What's hot (8)
Viewers also liked
Viewers also liked (18)
Similar to Cardiovascular System Problems in GP
Similar to Cardiovascular System Problems in GP (20)
More from rajendra deshpande
More from rajendra deshpande (20)
Recently uploaded
Recently uploaded (20)
Cardiovascular System Problems in GP
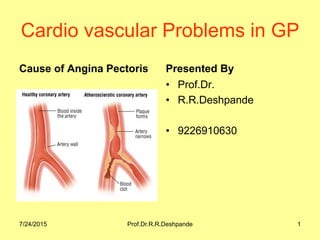
- 1. Cardio vascular Problems in GP Cause of Angina Pectoris Presented By • Prof.Dr. • R.R.Deshpande • 9226910630 7/24/2015 Prof.Dr.R.R.Deshpande 1
- 2. 7/24/2015 Prof.Dr.R.R.Deshpande 27/24/2015 Prof.Dr.R.R.Deshpande 2 Cardio vascular Problems in GP • Presented By – • Prof.Dr.R.R.Deshpande (M.D in Ayurvdic Medicine & M.D. in Ayurvedic Physiology) • www.ayurvedicfriend.com • Mobile – 922 68 10 630 • Mailme.drrrdeshpande@rediffmail.com
- 3. 7/24/2015 Prof.Dr.R.R.Deshpande 3 GP problems of CVS • 1) Acute chest Pain • • 2) hypertension • 3) Palpitation • 4) CCF
- 4. 7/24/2015 Prof.Dr.R.R.Deshpande 4 Acute chest Pain : • Cardiac Pain • a) IHD • b) MI • Non Cardiac pain • a) Respiratory • b) Oesophago – gastric • c) Chest wall • d) functional psychological (cardiac neurosis) • Neurosis : like a Benign tumour of the mind.
- 5. 7/24/2015 Prof.Dr.R.R.Deshpande 5 Cardiac Pain : • Chest pain = cardiac pain unless proved otherwise • Diagnosis is confirmed by ECG and other symptoms • Symptoms : retro sternal pain – constricting pain shown by clenched fist. • Cardiac Neurosis – Neurosis is like Benign Tumor of mind
- 6. 7/24/2015 Prof.Dr.R.R.Deshpande 6 IHD : Ischaemic Heart Disease • Causes : • 1) Less O2 supply : Arteriosclerosis – arteries – layer means tunica intima are rough • Atherosclerosis : Deposition of cholesterol on rough arteries. • IHD is caused by less O2 supply or increased demand of O2 due to LVH in chronic hypertension or vascular spasm
- 7. 7/24/2015 Prof.Dr.R.R.Deshpande 7 Angina Pectoris • 3 types according to duration and intensity. • 1) Stable or classical Angina • 2) Unstable angina • 3) M.I.
- 11. 7/24/2015 Prof.Dr.R.R.Deshpande 11 Stable angina Pectoris • Due to transient ischaemia – caused by vascular spasm – recovers by rest. • Pain is lasts for maximum 2-5 mins.
- 12. 7/24/2015 Prof.Dr.R.R.Deshpande 12 Unstable Angina (Pre infarction) • More severe, lasts longer • Due to transient blood loss, fissuring and disruption of Atheromatous plaque, forming a thrombus. • When Thrombolysis occurs, crisis ends. • If thrombus not dissolve & coronary artery is occluded – Necrosis of cardiac tissues occurs then heart attack occurs (MI)
- 13. 7/24/2015 Prof.Dr.R.R.Deshpande 13 Stable or classical Angina • i) Generally it occurs between age 50 – 60 years • ii) Acute chest pain : radiating towards • a) left shoulder b) Ulnar surface of hand and arm c) back d) neck e) jaw
- 14. 7/24/2015 Prof.Dr.R.R.Deshpande 14 Stable or classical Angina • Precipitating factors • 1) Hurriedly climbing up steps • 2) Heavy meal • 3) Anxiety and stress • 4) Straining for defecation • 5) After sexual intercourse
- 15. 7/24/2015 Prof.Dr.R.R.Deshpande 15 Stable or classical Angina • Treatment during attack • Relieved by a) Complete rest – for 2-5 mins. • Short acting Nitrates -- Glyceryl trinitrate – (Angised) 0.5 mg or Isosorbide dinitrate 5 mg (Tab Sorbitrate) or Nitroglycerine spray • Once the pain stops – spit or swallow tab • Throbbing headache – side effect
- 16. Stable & Unstable Angina 7/24/2015 16Prof.Dr.R.R.Deshpande
- 17. 7/24/2015 Prof.Dr.R.R.Deshpande 17 Stable or classical Angina • Nifedepine (Cap Depin)10 mg – • bitten by the patient – releases the liquid ( absorbed sublingualy)
- 18. 7/24/2015 Prof.Dr.R.R.Deshpande 18 Atypical presentation of Angina pectoris • i) Anginal decubitus : This pain occurs at night, when the patient is recumbent. • ii) Varient Angino or Prinz metal's angina : Chest pain at rest with palpitation and breathlessness.
- 19. 7/24/2015 Prof.Dr.R.R.Deshpande 19 Atypical presentation of Angina pectoris • iii) Wenback's second wind Angina : Pain starts white / after walking pain stops spontaneously without vasodialators.
- 20. 7/24/2015 Prof.Dr.R.R.Deshpande 20 Stable or classical Angina • 1) ECG should be taken during exercise called stress test or treadmill test. • ST depression in lead II or V1 to V6. suggests Ischaemia • 2) 2D Echo : To see the how much damage cardiac tissues. see the EF – Ejection faction if it is less than 50 % then suggest weak heart
- 21. 7/24/2015 Prof.Dr.R.R.Deshpande 21 Stable or classical Angina • 3) Angiography : To see whatever the damage is due to coronary artery block or not and to see the which vessel block and how many blocks are there. • Angiograpy is imp. to know whether the disease is • 1) One vessel, 2) Two vessel 3) Three vessel – Then CABG (Case is serious)
- 22. 7/24/2015 Prof.Dr.R.R.Deshpande 22 Prevention of Anginal Attacks : • 1) Modification of life style : • 2) Avoid the risk factors • 3) Adequate rest • 4) Proper exercises which will not precipitate to M.I. (Breathing, yogic exercises – best)
- 23. 7/24/2015 Prof.Dr.R.R.Deshpande 23 Prevention of Anginal Attacks • 1) Planning and time table • 2) Fatty food , high calorie diet, excessive sweets, chocolates should be avoided • 3) Rest – Rule of 8 -- 8 hours hobbies and with family, 8 hours sleep & rest , 8 hours for bread butter (job)
- 24. 7/24/2015 Prof.Dr.R.R.Deshpande 24 Prevention of Anginal Attacks • Drugs : • a) Nitrates • • b) blockers • • c) Ca antogonists • d) Anti-platelet
- 25. Treatment of Angina 7/24/2015 25Prof.Dr.R.R.Deshpande
- 26. 7/24/2015 Prof.Dr.R.R.Deshpande 26 Nitrates : Coronary vaso-dialators • 1) Glyceryl trinitrate – short acting (Tab Angised ) or • 2) Long acting Isosorbide Dinitrate – (Isordil or sorbitrate ) 5 mg 8 hourly or • 3) Isosorbide 5 mononitrate (Ismo 20 or Monotrate 20 mg tds • GIN – Glycerl trinitrate ointment or Transdermal patches
- 27. 7/24/2015 Prof.Dr.R.R.Deshpande 27 -blockers • Reduce the oxygen requirement of heart by reducing HR & BP and myocardial contractility. • • Atenelol – Tab Aten – 25-100 mg / day.OD • Should be started along with Nitrates
- 28. 7/24/2015 Prof.Dr.R.R.Deshpande 28 Ca Antagonists • This is powerful coronary and peripheral vaso-dialator. • Therefore give increase or adequate O2 supply and reduced O2 requirement. • Blocks the entry of Ca into myocardial cells. • Therefore reduced the contractivity.
- 29. 7/24/2015 Prof.Dr.R.R.Deshpande 29 Ca Antagonists No Name Dose 1 Nifedipine (Cap Depin,Calcigard) 10 to 40 mg TDS 2 Amlodipine(Tab Amlogard) 5– 10 mg OD 3 Verapramil(Tab Isoptin) 80-120 mg TDS 4 Diltiazem (Tab Dilzem) 30—90 mg TDS
- 30. 7/24/2015 Prof.Dr.R.R.Deshpande 30 Anti – Platelet • Thrombus dissolving action. • Aspirin – Acytel – calycitric acid – Its powerful analgesic. • Tab – Aspirin also known as 'Magic bullet' for heart patient • Doses – 100 – 150 mg/day.(Disprin) • Inhibit the aggregation of platelets. • Cheap & proved effective • Well understood side effect profile.
- 31. 7/24/2015 Prof.Dr.R.R.Deshpande 31 Anti – Platelet -- Contraindication • 1) In peptic ulcer & 2) Hypersensitivity patients. • For this patients • 1) Tyclopidine 250 mg – BD (Tab – Tyklid) • Side effects : effect starts after 5 days. • Neutropenia – So Adv Haemogram per week. • 2) Clopidogrel – (Tab – clopiget) 350 mg – stat & 75 mg BD.
- 32. Ayurvedic Advice for Angina • Rule out the cause and treat accordingly e.g. anemia, syphilis, hyper thyroidism, paroxysmal tachycardia. • Advise obese to reduce weight. • Keep away from bad habits like smoking, alcohol, tobacco,excessive coffee or tea etc. • Control diabetes and hypertension with proper medication. • Do not exert too much. Have enough rest 7/24/2015 Prof.Dr.R.R.Deshpande 32
- 33. Ayurvedic Advice for Angina • Do not suppress or force natural urges like urine and stool. • Regular bowel movements. • Avoid over indulgence of sex. • Avoid excessive sweat, sour and salty food. 7/24/2015 Prof.Dr.R.R.Deshpande 33
- 34. Ayurvedic Medicines for stable Angina • Bruhat Vatachintamani 30-60 mg. with ginger juice. • Harinshrung Bhasma 175 mg. + Laxmivilas 50 mg. with ginger juice 7/24/2015 Prof.Dr.R.R.Deshpande 34
- 35. Prevention of progress of Angina • For prevention use following for 3 months • Makardhwaja 60 mg. + Shrung Bhasma 125 mg. each morning and Mahalaxmivilas 125 mg. + Sitopaladi Churna 750 mg. afternoon and night. 7/24/2015 Prof.Dr.R.R.Deshpande 35
- 36. 7/24/2015 Prof.Dr.R.R.Deshpande 36 Unstable Angina or Pre Infarction Syndrome • Known case of stable Angina – In this case if • 1) Pain more severe, last longer, occur with increasing frequency. • 2) Pain occurs at rest kin known case of stable Angina. • 3) Pain associated with vomiting, dyspnoea & perspirations. • 4) Pain not relieved completely by sublingual nitrates.
- 37. 7/24/2015 Prof.Dr.R.R.Deshpande 37 Unstable Angina or Pre Infarction Syndrome • Diagnosis : Transient ECG changes – This are 'ST" elevation / depression and 'T' Inversion. • Changes revert back to normal in 24 hours. • Since No necrosis • Suspect MI when ? • 1) ECG changes no revert back in 24 hours. • Cardiac enzymes levels are increased
- 38. 7/24/2015 Prof.Dr.R.R.Deshpande 38 Unstable Angina or Pre Infarction Syndrome • For the Heparinization admit the patient. Its also called – Thrombolytic Therapy. • Give Inj – Streptokinase (I/V) or Urokinase
- 39. Coronary Arteries 2 7/24/2015 39Prof.Dr.R.R.Deshpande
- 40. 7/24/2015 Prof.Dr.R.R.Deshpande 40 Acute M.I. • Symptoms : 1) Severe retrosternal constricting chest pain – radiating. • Infrascapular (back pain) • Left shoulder, jaw, neck & epigastrium • Vomitting / Nausea • Profused sweating • Incontinance of urine or stool • (Complete rest even – bed pan gives on bed)
- 41. 7/24/2015 Prof.Dr.R.R.Deshpande 41 Acute M.I. • Sympathetic stimulation --- • Tachycardia, palpitation, restlessness, sweating. • Parasympathetic stimulation --- • Bradycardia and hypotension
- 42. 7/24/2015 Prof.Dr.R.R.Deshpande 42 Atypical M.I. or Silent Inforct • 1) No pain in long standing DM, HT, elderly or middle aged post-operative patient. • 2) Sudden sweating and vomiting, with or without chest pain. • 3) Sudden breathlessness with or without chest pain. • 4) Acute confusion , severe unexplained, weakness, arrhythmia, syncope, sudden death
- 43. 7/24/2015 Prof.Dr.R.R.Deshpande 43 How you can diagnose the pain of M.I. ? • Patient is restless • Moving on bed. • Profuse sweating, cold extrimities. • Anxious, pale – Face • Pulse – Brady or Trachy or Normal • B. P. -- Hypo or Hyper or normal
- 44. 7/24/2015 Prof.Dr.R.R.Deshpande 44 Acute M.I. • If there is doubt then repeat the ECG. • RS – Brasal creptitions • ECG – i) ST elevation, but • ii) After 24 hours – 'T' inversion
- 45. Types of MI 7/24/2015 45Prof.Dr.R.R.Deshpande
- 47. Area of Infarct 7/24/2015 47Prof.Dr.R.R.Deshpande
- 48. MI – ST Elevation 7/24/2015 48Prof.Dr.R.R.Deshpande
- 49. Area of Infarct Table 7/24/2015 49Prof.Dr.R.R.Deshpande
- 50. 7/24/2015 Prof.Dr.R.R.Deshpande 50 Acute M.I. -- Blood investigations • 1) CPK – MB • 2) SGOT • 3) LDH • 4) Cardiac Froponin – T (with 5 hours) costly but confirmatory. • 5) Sr. Myoglobin – very sure if it is positive. • Above all enzymes are in the enzymes come from cardiac necrosed tissue. In blood this enzymes level increases. • When there is muscle degeneration when level of SGOT is increased.
- 51. 7/24/2015 Prof.Dr.R.R.Deshpande 51 Acute M.I. --Before hospitalization : • 1) Sublingual – Tab Angised 0.5 mg or Tab Sorbitrate 5 mg. • 2) To dissolve the thrombus– Disprin 100 – 150 mg. • 3) For severe pain – Inj. Fortwin – 30 mg I/M • 4) When bradycardia due to cardiac shock then gives Inj – Atropin 0.3 to 0.6 mg I/V • 5) In known patient of LVH gives – Inj – Lasix 20 – 80 mg I/V diuretics) • If B.P. falls down rapidly -- Shift the patient immediately in the hospital
- 53. ECG Changes in MI 7/24/2015 53Prof.Dr.R.R.Deshpande
- 54. Ayurvedic Medicines after Acute attack of MI • For stable patients : Use following medicines • (1) Bruhatvatachintamani Rasa 1 Tab. 2 times a day. • (2) Shrungabhasma 250 mg. 3 times a day. • (3) Vatavidhvansa Rasa 2 Tab. 3 times a day. • (4) Khurasanai Ova 100 mg. 3 times a day. • (5) Prasham 4 tablespoon with equal amount of water at bed • time. • (6) Triphala Churna 1 tablespoon with warm water at bed time. 7/24/2015 Prof.Dr.R.R.Deshpande 54
- 55. Prevention of further Heart Attack • 1) Suvarnabhasma 6 mg. + Makardhwaja 50 mg. + Shrungabhasma 250 mg. 2 times a day with honey. Or • 2) Hrudayanarva Rasa (B) 1 Tab. 2 times a day +Nagarjunabhra Rasa 2 Tab. 3 times a day + Yakuti Rasa 2 Tab. 3 times a day+ Prabhakar Vati 2 Tab. 3 times a day. 7/24/2015 Prof.Dr.R.R.Deshpande 55
- 56. 7/24/2015 Prof.Dr.R.R.Deshpande 56 Hypertension • Mild – 90 – 110 mm of Hg. • Moderate – 110 – 130 mm of Hg • Severe - > 130 mm of Hg
- 57. Rheumatic Mitral Stenosis 7/24/2015 57Prof.Dr.R.R.Deshpande
- 58. Dial BP Apparatus – Visiting Bag 7/24/2015 58Prof.Dr.R.R.Deshpande
- 59. Damage by Hypertension 7/24/2015 59Prof.Dr.R.R.Deshpande
- 60. 7/24/2015 Prof.Dr.R.R.Deshpande 60 Hypertension • 1) Most of the hypertension is Idiopathic. • 2) Secondary Hypertension – Renal RFT • Hepatic – USG, LFT • adv. 2D Echocardiogram – Cardiac – Valvular defect • Acc. to symptoms – hormonal (T3, T4, T3H etc) • RFT – Renal Function Test -- Urea, Creatinine • In every Hypertension patient adv. – USG of abdomen and some time Renal angiography
- 62. 7/24/2015 Prof.Dr.R.R.Deshpande 62 Hypertension -- Treatment • Mild hypertension – No Drug treatment. • Life style management – Planning, time management. • Reduced stress – Meditation, Yoga, Pranayam • Restriction of Salt, pickle, papad, fast food, and preservative foods, wafers all are restricted.
- 63. Hypertension -- Treatment • Deep fried food are avoided and unsaturated oil use e.g. sunflower oil • Regular walking – Collateral circulation are develops. • Reduced weight if high weighs. • Stops alcohols, tobacco, cigars etc 7/24/2015 Prof.Dr.R.R.Deshpande 63
- 64. 7/24/2015 Prof.Dr.R.R.Deshpande 64 Hypertension -- Treatment • Monodrug Therapy 1) - Blockers • Tab – Aten – 25 – 50 mg & 100 mg – 1 – 0 – 0 • 2) Ca – channel blocker • Tab – Stamlo 2.5, 5 mg – 1 – 0 – 0 • 3) ACE – Inhibitor Tab – Enam – 5 to 10 mg.
- 65. 7/24/2015 Prof.Dr.R.R.Deshpande 65 Moderate Hypertension -- Treatment • Mono drug – Maximum dose or Combination treatment • Either - Blocker + Ca chanel blocker or (minimum dose) - Blocker + ACE inhibitor • Compliance of patient is very imp. + Diuretic – Lasix 40 mg 1 OD.
- 66. Moderate Hypertension -- Treatment • Kesol – To avoid lasix's side effect • Diuretic drugs – Potassium sparing diuretics • Tab- Biduret, Tab – Lasilactone - diurectics 7/24/2015 Prof.Dr.R.R.Deshpande 66
- 67. 7/24/2015 Prof.Dr.R.R.Deshpande 67 Severe Hypertension • Malignant H. T. • Medical Emergency • Admit instant -- Treatment is of hospital level • Symptoms : • 1) Severe Headache • 2) Vomiting • 3) Visual • 4) Convulsions, paralysis (transient) • 5) Coma
- 68. 7/24/2015 Prof.Dr.R.R.Deshpande 68 Accelerated H. T. • Medical urgency • At level of G.P. (No serious complaint of patient) • Diastolic > 130 , but without symptoms like in Malignant HT, which you can treat primarilty • Cap – Depin – 5 mg gives sublingulal, repeat after 10 mins, till the B.P. comes to 110.
- 69. 7/24/2015 Prof.Dr.R.R.Deshpande 69 Accelerated H. T. • Then cap – Depin 10 mg TDS (1 – 1 – 1) • Tab Aten – 50 mg BD • Tab- Lasix – 40 mg BD • If the BP doesn’t come down 110 within 24 hours then admit the patient.
- 70. Ayurvedic Medicines for Hypertension • Hypertension ( Pitta avruta vata) – • Duralabhadi ( Dhamasa) Kadha -- 4 tsf with equal amount of water BD • 7/24/2015 Prof.Dr.R.R.Deshpande 70
- 71. Ayurveda for Mild Hypertension • Diastolic less than 90 mm of Hg • (i) Siledin ( Alarsin ) 2 Tab. 3 times a day. • (ii) Sapera forte (charak ) 2 tab. at bed time. 7/24/2015 Prof.Dr.R.R.Deshpande 71
- 72. Ayurveda for Moderate Hypertension • Diastolic in-between 90-100 mm of Hg • (i) Abana 2 Tab. 3 times a day. And • (ii) Punanarnavasava 4 tablespoon with equal amount of water 2 times after meals. 7/24/2015 Prof.Dr.R.R.Deshpande 72
- 73. Ayurveda for Severe Hypertension • Diastolic more than 100 mm of Hg • Suvarna Sutshekhar 30 mg with honey every 5 minutes. • Rasagandha (AYR) 2 Tab. 3 times a day. • Sutshekhar Rasa sadha 2 Tab. 3 times a day. • Arogyavardhini 2 Tab. 3 times a day. • Duralabhadi kwath 4 tablespoon with equal water 2 • times after meals. 7/24/2015 Prof.Dr.R.R.Deshpande 73
- 74. Ayurveda for Severe Hypertension • Diastolic more than 100 mm of Hg • Arogyavardhini 2 Tab. 3 times a day. • Gokshuradi Guggulu 2 Tab. 3 times a day. • Rasayana Churna (HP) 1 tablespoon 2 times a day. • Siledin (A) 2 Tab. at bed time 7/24/2015 Prof.Dr.R.R.Deshpande 74
- 75. Vaman – Useful to reduce Cholesterol • High Cholesterol like above 300 mg % -- cause Atherosclerosis – leads to Hypertension • Diet control + Lovastatin like medicines can reduce cholesterol very slowly like 20 mg in 6 months • But Vaman ( Therapetic Vomition ) with prior Snehapan with Tiktak Ghee 50 mg daily + Fomentation ,can show magic results for reducing Blood Cholesterol level + Internally • Tab Arogyavardhini 3 TDS + Tab Triphala 1 TDS + Nagarmotha & Vidanga churna each 3 Gm TDS 7/24/2015 Prof.Dr.R.R.Deshpande 75
- 76. 7/24/2015 Prof.Dr.R.R.Deshpande 76 Palpitation • 1) Cardiac – Paroxysmal ventricular Tachyeardia or Extrasyslole (Take history) • 2) Non cardiac – i) Hyperthyroidism ii) Hypoglycemia • 3) Functional – Cardiac Neurosis (Psychological)
- 79. 7/24/2015 Prof.Dr.R.R.Deshpande 79 Palpitation • Tab – Ativan (Lorazepam) – 1 mg stat – BD for 4 days • Tab – Inderal – 10 – 40 mg TDS • Also a anti anxiety or anti stress drug. Therefore Anti Arrythmic (acts physically and mentally also)
- 80. 7/24/2015 Prof.Dr.R.R.Deshpande 80 Hyper & Hypoglycemia • Diabetic ketoacidosis – Hyper glycemia (fruity odour) • Hypoglycemia is always fatal because brain can dead within 2 min if less or no supply of glucose. • Insulin dependent patient ,if do fasting. • Profuse sweating and acute incidence. • Give the I/V glucose – 25 %
- 81. 7/24/2015 Prof.Dr.R.R.Deshpande 81 CCF – Congestive Cardiac Failure or Cardiac Asthma • LVF (Left Ventricular Failure) • RVF (Right Ventricular Failure) • Cardiac Asthma is the breathlessness , during CCF.
- 82. Symptoms of CCF 7/24/2015 82Prof.Dr.R.R.Deshpande
- 83. Symptoms of CCF 2 7/24/2015 83Prof.Dr.R.R.Deshpande
- 84. 7/24/2015 Prof.Dr.R.R.Deshpande 84 CCF • Treatment At GP level • 1) Bed rest completely • 2) Salt free diet (because of salf is hygroscopic nature) • 3) Fluid intake restricted (Inj. Lasix – 40 mg stat. or tab lasix – 40 mg BD)
- 85. CCF • liq. Kesol – 1 TSF – TDS with glass of water. • or pattasium soarina diuretics are used such as • Tab Amifru – 1 – OD or • Tab Lasilactone – 1 – OD 7/24/2015 Prof.Dr.R.R.Deshpande 85
- 86. 7/24/2015 Prof.Dr.R.R.Deshpande 86 CCF • For the heart : • Lanoxin – 0.25 mg 1 OD for 6 days (Sunday off) • Inj – Aminophylline 10 ml diluted in 20 ml of 25 % dextrose. • This inj.-- give very very slow (for 30 ml – 10 min)
- 87. Congestive Heart Failure 7/24/2015 87Prof.Dr.R.R.Deshpande
- 88. 7/24/2015 Prof.Dr.R.R.Deshpande 88 CCF • B.P. control – Tab Enam 2.5 mg BD (Enalapril) • Infection – control by Cap – Ampiclox – 50 mg TDS • If till there is no control then give adv. for Hospitalisation
- 89. Ayurvedic Medicines for CCF • Shrungbhasma 2 Tab. 3 times a day. • Vishatindookvati 1 Tab. 3 times a day. • Punarnavasava 4 tablespoon with equal amount of water 2 times after meals. 7/24/2015 Prof.Dr.R.R.Deshpande 89
- 90. Ayurvedic Cardiac Tonic • 1) Arjunarishta(Parthadyarishta) -- 4tsf with equal amount of water BD in CCF • 2) Arjun Kshirpak --- 50 ml BD in patients of Angina Pectoris 7/24/2015 Prof.Dr.R.R.Deshpande 90
- 91. X ray of CCF 7/24/2015 91Prof.Dr.R.R.Deshpande
- 92. Shock ,Pulse less patient • Shock,Pulse less patient ---- • In Emergency Life saving drugs in Ayurveda – • Tab Laxmi vilas rasa • Hemagarbha Chatan or licking 7/24/2015 Prof.Dr.R.R.Deshpande 92
- 93. Conducting system of Heart 7/24/2015 93Prof.Dr.R.R.Deshpande
- 94. Ayurved & Yoga – Good help for Heart Patients • Ayurvedic Internal Medicines • Ayurvedic Detox Therapies or Panchakarma & allied procedures • Yoga Asanas • Pranayam • Meditation • Everything can be helpful for Heart patients ,but always under guidance of Expert 7/24/2015 Prof.Dr.R.R.Deshpande 94
- 95. Abhyanga • Gentle ,soft Full body massage helps to improves Blood circulation, Providing good nutrients to cells, remove the waste products efficiently • Soothening to body & Mind 7/24/2015 Prof.Dr.R.R.Deshpande 95
- 96. Shirodhara – Beneficial to reduce Blood pressure • Oil shower on head controls hyper activity of sympathetic system • Reduces stress • Cool down irritability of mind • Produce sound sleep 7/24/2015 Prof.Dr.R.R.Deshpande 96
- 97. Hrud Basti – Heart Tonic • Improves tone of Cardiac muscle • Improves elasticity of vessels • Very Good Analgesic & Anti-inflammatory action • Reduces Anginal pain 7/24/2015 Prof.Dr.R.R.Deshpande 97
- 98. Raktamokshan or Blood letting – Good to reduce Hypertension • Reduces blood volume • Reduces cardiac load • Stimulation for proper blood circulation • Removes Impurities or Ama or Endo toxins from blood 7/24/2015 Prof.Dr.R.R.Deshpande 98
- 99. Pranayam –Deep breathing Practice • Proper perfusion of Oxygen • More Energy to cardiac muscle • Heart function improves 7/24/2015 Prof.Dr.R.R.Deshpande 99
- 100. Meditation – Best Relaxation • Best way for maintaining Homeostasis • Physical Rest • Mental Tranquility 7/24/2015 Prof.Dr.R.R.Deshpande 100
- 101. Yoga Postures for Heart Patients 7/24/2015 Prof.Dr.R.R.Deshpande 101
- 102. Yoga Postures for Heart Patients 7/24/2015 Prof.Dr.R.R.Deshpande 102
- 103. Yoga Postures for Heart Patients 7/24/2015 Prof.Dr.R.R.Deshpande 103
- 104. 7/24/2015 Prof.Dr.R.R.Deshpande 104 Ayurved for General Practioner • Very very popular Book in Medical Practioners • 100 common symptoms of General Practice with causes,Investigations & Ayurvedic Treatments
- 105. 7/24/2015 Prof.Dr.R.R.Deshpande 105 Clinical Examination • Systemic Examination of 8 systems • Ayurvedic Srotas Examination • Clinical significance of Lab Tests & Radiology,USG,2D Echo
- 106. 7/24/2015 Prof.Dr.R.R.Deshpande 106 Notes on Medicine Part 1 • Very very useful Book for all Medical Practioners • Guidelines with causes,symptoms,Ay urvedic & Modern Treatments to treat Fever,Pain in Abdomen & Arthritis
- 107. 7/24/2015 Prof.Dr.R.R.Deshpande 107 Best Book for Medical Students & Practioners
- 108. Preventive Cardiology & Ayurvedic Management • Best Book for GP • All cardiac problems like Hypertention,CCF, Angina,Myocardial Infarct are discussed with Ayurvedic Management Contact -922 68 10 630 7/24/2015 Prof.Dr.R.R.Deshpande 108
- 109. Digestive Problems & Ayurvedic Management • Best Book for GP • All Digestive problems like Acidity,Pain in abdomen, • Constipation ,colitis are discussed with Ayurvedic Management Contact -922 68 10 630 7/24/2015 Prof.Dr.R.R.Deshpande 109
- 110. Gynaecological Problems & Ayurvedic Management • Best Book for GP • All Gynaecological problems like Heavy bleeding,White discharge,Infertility,ca ncer are discussed with Ayurvedic Management Contact -922 68 10 630 7/24/2015 Prof.Dr.R.R.Deshpande 110
- 111. Arthritis,Backache & Ayurvedic Management • Best Book for GP • All Joint problems like Rheumatoid Arthritis,Osteoarthritis ,Backache are discussed with Ayurvedic Management Contact -922 68 10 630 7/24/2015 Prof.Dr.R.R.Deshpande 111
- 112. Neurological Problems & Ayurvedic Management • Best Book for GP • All Neurological problems like Headache,Epilepsy,Al zeimer’s Disease are discussed with Ayurvedic Management Contact -922 68 10 630 7/24/2015 Prof.Dr.R.R.Deshpande 112
- 113. Ayurvedic Concept of Diet & Nutrition • Best Book for GP • Dietary Advice according to Prakruti ,Dietary prescriptions for many diseases are given • Contact -922 68 10 630 7/24/2015 Prof.Dr.R.R.Deshpande 113
- 114. Health Tips for 365 Days 7/24/2015 Prof.Dr.R.R.Deshpande 114 • This Book is very useful from Common man to Doctors • It covers all imp aspects mentioned in Ayurveda • Open as per date & complete reading of one page only
- 115. Prof.Dr.Deshpande’s Popular Links on Internet • Just Start Internet on Desk top or Lap top or on your mobile . Copy Following Link & Paste as Web address –URL • http://www.youtube.com/user/deshpande1 959 • http://www.slideshare.net/rajendra9a/ • http://www.mixcloud.com/jamdadey/ 7/24/2015 Prof.Dr.R.R.Deshpande 115
- 116. Prof.Dr.Deshpande’s Popular Links on Internet • Just Start Internet on Desk top or Lap top or on your mobile . Copy Following Link & Paste as Web address –URL • http://professordeshpande.blogspot.in • http://professordrdeshpande.blogspot.in/ • http://www.mixcloud.com/rajendra- deshpande • https://soundcloud.com/professor- deshpande 7/24/2015 Prof.Dr.R.R.Deshpande 116
- 117. Prof.Dr.R.R.Deshpande • Sharing of Knowledge • FOR • Propagating Ayurved 7/24/2015 117Prof.Dr.R.R.Deshpande