Ano rectal problems ppt
•
83 likes•7,941 views

Anorectal Problems - PPT By Prof. Dr. R. R. Deshpande • This PPT has following contents – 1) Anatomical Aspect 2) Acute Constipation 3) Chronic Constipation 4) Congenital problems 5) Anal Stenosis 6) Anorecatl agenesis 7) Piles 8) Fissure in Ano 9) Fistula in Ano 10) Prolapse of Rectum 11) Pilonidal Sinus 12) Stricture of Anus & Rectum 13) Condyloma 14) Carcinoma of Rectum 15) Pruritus Ani 16) Ano Rectal pain 17) Anal Incontinence 18) Proctitis 19) Rectal Polyp 20) Ayurvedic Treatments • Visit – www.ayurvedicfriend.com • Phone – 922 68 10 630

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ano rectal problems ppt
Similar to Ano rectal problems ppt (20)
More from rajendra deshpande
More from rajendra deshpande (20)
Recently uploaded
Recently uploaded (20)
Ano rectal problems ppt
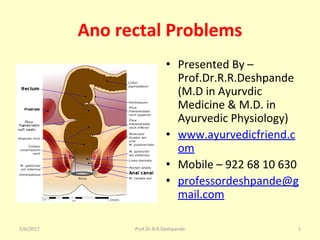
- 1. Ano rectal Problems • Presented By – Prof.Dr.R.R.Deshpande (M.D in Ayurvdic Medicine & M.D. in Ayurvedic Physiology) • www.ayurvedicfriend.c om • Mobile – 922 68 10 630 • professordeshpande@g mail.com 2/6/2017 Prof.Dr.R.R.Deshpande 1
- 2. Contents of this PPT • 1) Anatomical Aspect • 2) Acute Constipation • 3) Chronic Constipation • 4) Congenital problems • 5) Anal Stenosis • 6) Anorecatl agenesis 2/6/2017 2Prof.Dr.R.R.Deshpande
- 3. Contents of this PPT • 7) Piles • 8) Fissure in Ano • 9) Fistula in Ano • 10) Prolapse of Rectum • 11) Pilonidal Sinus • 12) Stricture of Anus & Rectum 2/6/2017 3Prof.Dr.R.R.Deshpande
- 4. Contents of this PPT • 13) Condyloma • 14) Carcinoma of Rectum • 15) Pruritus Ani • 16) Ano Rectal pain • 17) Anal Incontinence • 18) Proctitis • 19) Rectal Polyp • 20) Ayurvedic Treatments 2/6/2017 4Prof.Dr.R.R.Deshpande
- 5. Anatomy of Anorectal region – Rectum • Distal part of colon .Sogmoid colon above & anal canal below • 3 cardinal features ( Taeniae coli , Haustrations, Appendices epiploicae ) of colon are absent • Pelvic organ – situated in posterior part of lesser pelvis – in front of lower 3 sacral vertebrae 2/6/2017 5Prof.Dr.R.R.Deshpande
- 6. Anatomy of Anorectal region – Rectum • Diameter – 5 inches .Lower part is dilated to form Rectal Ampulla • Lower 1/3rd of rectum is devoid of peritoneum • Fold of peritoneum between –urinary bladder & rectum ,in males – Recto vesical pouch • Fold of peritoneum between – Uterus ,cervix ,vagiba & rectum ,in Females – Recto uterine pouch 2/6/2017 6Prof.Dr.R.R.Deshpande
- 7. Anatomy of Anorectal region – Rectum • Blood supply – Superior rectal ,Medial rectal, Median sacral artery • Venous drainage – Superior & Middle rectal vein • Nerve supply – Sympathetic from L1 & 2 , Parasympathetic from S 2,3,4 2/6/2017 7Prof.Dr.R.R.Deshpande
- 8. Anatomy of Anorectal region – Rectum • Applied Anatomy – • PR Examination for BPH etc • Examination of Rectal mucosa – Proctoscopy or Sigmoidoscopy • Prolapse of Rectum – Rectum comes out through anus 2/6/2017 8Prof.Dr.R.R.Deshpande
- 9. Anatomy of Anal canal • Terminal part of colon .Situated below the Pelvic diaphragm ,in anal triangle of peritoneum ,between right & left ischio rectal fossa .3.8 cm long .Extends from Ano rectal junction to anus • 3 parts – Upper mucous part ,Middle transitional zone, Lower cutaneous part 2/6/2017 9Prof.Dr.R.R.Deshpande
- 10. Anatomy of Anal canal • 1 . Upper mucous part – 15 mm long ,lined by mucous membrane .Mucous membrane shows 6 to 10 vertical folds – Anal column • Lower end of anal column are united to each other by transverse fold of mucous membrane = Anal valves • Anal valves together forms ,a transverse line = Pectinate line 2/6/2017 10Prof.Dr.R.R.Deshpande
- 11. Anatomy of Anal canal • 2 . Middle part or Transitional zone – 15 mm long ,Do not contain anal columns . • White line of Hilton = Lower limit of Pecten 2/6/2017 11Prof.Dr.R.R.Deshpande
- 12. Anatomy of Anal canal • 3 . Cutaneous part -- 8 mm long .Contain sweat & sebaceous glands • Muscles of Anal canal – Internal anal sphincter ( Involuntary) & External anal sphincter ( Voluntary) – subcutaneous part , superficial part , deep part 2/6/2017 12Prof.Dr.R.R.Deshpande
- 13. Anatomy of Anal canal • Nerve supply –External anal sphincter – supplied by Inferior rectal nerve & 4th sacral nerve • Blood supply --- Anal canal ,above the Pectinate line is supplied by – superior rectal artery & below the pectinate line by – Inferior Rectal artery 2/6/2017 13Prof.Dr.R.R.Deshpande
- 14. Anatomy of Anal canal • Venous drainage – • 1.Internal Rectal venous plexus • ( Haemorrhoidal Plexus ) – Lies in submucosa of the anal canal .Drains into superior rectal vein .Internal rectal venous plexus is an important site of Porta caval Anastomasis • The veins present at 3 ,7 & 11 o clock are potential sites for primary Internal piles 2/6/2017 14Prof.Dr.R.R.Deshpande
- 15. Anatomy of Anal canal • External Rectal venous plexus – Freely communicates with the Internal rectal venous plexus • Anal veins – Arranges radially around the anal margin .Excessive straining during defaecation rupture the anal veins – forms sub cutaneous haematoma = External Piles 2/6/2017 15Prof.Dr.R.R.Deshpande
- 16. Anatomy of Anal canal • Applied Anatomy – • 1.Internal or True Piles – Dilation of Internal Rectal venous plexus – classified into 2 groups • Primary True Piles – Dilation of Internal Rectal venous plexus at 3,7,& 11 o clock • Secondary True Piles – Dilation of other than above sites 2/6/2017 16Prof.Dr.R.R.Deshpande
- 17. Anatomy of Anal canal • Applied Anatomy – • 2. External or False Piles – Rupture of anal veins ,causing sub cutaneous haematoma .External Piles – No bleeding ,but painful • 3.Anal Fissure – Rupture of anal valve .Painful with blood sticked to faeces 2/6/2017 17Prof.Dr.R.R.Deshpande
- 18. Anatomy of Anus • 4.Fistula in Ano – Abnormal epithelized tract ,containing 2 cavities or 1 cavity with the exterior outer opening of anal canal .4 cm below & in front of tip of coccyx • Skin around anus is pigmented • Thrown into radiating folds .Contain ring of Apocrine gland – keeping anus moist with typical foul smell 2/6/2017 18Prof.Dr.R.R.Deshpande
- 19. 2/6/2017 Prof.Dr.R.R.Deshpande 19 Acute Constipation causes • 1) Local pain at anus – painful fissure, perianal abscess. • 2) Elderly bed ridden patient. • 3) Pregnancy. • 4) Constipation with colicky pain in abdomen,Board like rigidity, abdominal distention or vomiting- Intestinal obstruction. (hyper peristalsis) or paralytic ileus (No peristalsis) or Acute Abdomen. • 5) Idiopathic functional constipation.
- 21. 2/6/2017 Prof.Dr.R.R.Deshpande 21 Acute Constipation- Treatment 1 • 1) For perianal abscess – Incision & drainage. • 2) For fissure in Ano – - Local – Xylocaine oint. - Cap Mox – 500 mg TDS. - Tab Tini – 300 mg – 1 BD. - Tab Voveron – 100 mg – 1 BD. - Tab Triphala vati – 2 H.S.
- 22. 2/6/2017 Prof.Dr.R.R.Deshpande 22 Acute Constipation- Treatment 2 • 3) For idiopathic constipation – - Tab Herbolax (Himalaya) 3 H.S or Abhayaristha – 3 tsf with equal quantity of water-BD. • 4) For Acute Abdomen – - Admit Immediately.
- 23. 2/6/2017 Prof.Dr.R.R.Deshpande 23 Chronic Constipation – causes 1 (Habitual Constipation) • Lack of exercise (especially abdominal muscle exercises – poor abdominal muscle tone.) • Lack of roughage (Green vegetables, fruits, raw bananas) in Diet.
- 24. 2/6/2017 Prof.Dr.R.R.Deshpande 24 Chronic Constipation causes 2 (Habitual Constipation) • Drinking Less water or beverages. • Tobacco, Mawa, smoking. • Drugs (Anti-hypertensives, antacids, Iron, NSAIDS).
- 25. 2/6/2017 Prof.Dr.R.R.Deshpande 25 Chronic Constipation causes 3 (Habitual Constipation) • Insulting Natural calls. • Pain at anus (Fissure, anal stricture, Growth). • Bed ridden patients
- 26. 2/6/2017 Prof.Dr.R.R.Deshpande 26 Chronic Constipation causes 4 (Habitual Constipation) • 4) In Elderly alternate constipation & Diarrhoea or Constipation with P /R bleeding ---- R / O -- Malignancy of colon or rectum • 5) Long term use of Laxatives or Enema( Loss of Muscle Tone)
- 27. Types of stool 2/6/2017 27Prof.Dr.R.R.Deshpande
- 30. Constipation – Takes much time to get sensation 2/6/2017 30Prof.Dr.R.R.Deshpande
- 31. Constipation – How much I should strain ? 2/6/2017 31Prof.Dr.R.R.Deshpande
- 32. Squatting & Constipation relation? 2/6/2017 32Prof.Dr.R.R.Deshpande
- 33. 2/6/2017 Prof.Dr.R.R.Deshpande 33 Chronic Constipation- Treatment • 1) Treat above said causes & Regular abdominal massage on empty stomach with warm sesame oil & fomentation. Regular 45 min walk, Pavanmuktasan, Naukasan • 2) Intermittent ayurvedic oil Enemata (Anuvasan Basti). Caution Elderly patient – alternate constipation & Diarrhea, with P/R bleeding – Rule out Rectal or colonic cancer.
- 34. Constipation –Causes & Effects Habit Effect Effect Final Effect Suppression of urge to defecate Contraction of External sphincter & associated muscles Absence of Bowel movement Constipation Inadequate fluid & water intake Increased intestinal transit time Increased reabsorption of water Constipation Chronic Anxiety Generalized muscle tension Decreased intestinal motility Constipation Inadequate physical exercise Decreased Muscle tone Decreased Peristalsis Constipation 2/6/2017 34Prof.Dr.R.R.Deshpande
- 36. Congenital Problems • 1) Post anal dermoid cyst • 2) Sacro-Coccygeal Teratoma • 3) Imperforated Anus 2/6/2017 36Prof.Dr.R.R.Deshpande
- 37. 1) Post anal dermoid cyst • Situated behind anus & in front of coccyx & sacrum. • May be seen in adults. • Soft cystic swelling • Cyst may get infected & sinus may form • Treatment - Excision 2/6/2017 37Prof.Dr.R.R.Deshpande
- 38. 2) Sacro-Coccygeal Teratoma • Teratoma at sacro-coccygeal region. • Most common Tumour seen in neonatal baby. • Firm in consistency • It is usually seen as a big swelling & may change into malignancy. • Treatment - Excision 2/6/2017 38Prof.Dr.R.R.Deshpande
- 39. 3) Imperforated Anus • Common congenital abnormality • Imperfect fusion of a hind-gut & lower part of anal canal (proctodeum) 2/6/2017 39Prof.Dr.R.R.Deshpande
- 40. Anal stenosis • The whole of anal canal is narrow or anus is microscopic with a minute opening • The patient presents passing of a meconium with pain • Treatment - Regular dilatation of anus. 2/6/2017 40Prof.Dr.R.R.Deshpande
- 41. Narrow Anal opening 2/6/2017 41Prof.Dr.R.R.Deshpande
- 42. Ano-Rectal Agenesis • A blind rectal pouch lies just above the pelvic floor. • In the male the fusion is attached to bladder & often there is a fistula between rectum & bladder known as rectovesical fistula. • In females, fistula may be present with posterior fornix. • In this variety, sometimes gas or meconium is present in urine. 2/6/2017 42Prof.Dr.R.R.Deshpande
- 44. Recto vesical Fistula 2/6/2017 44Prof.Dr.R.R.Deshpande
- 45. Etymology of Haemorrhoid • Pile - Pila = ball = Round shape • Hemorrhoid --- • Haem = Blood & Orrhos = Oozing 2/6/2017 45Prof.Dr.R.R.Deshpande
- 46. Piles • Dilated plexus of hemorrhoidal veins in relation to anal canal • Inflammation of anal cushion • (Anal cushion is formed by venules, arterioles, arterio venule junction, smooth connecting tissues & mucosa of anal canal.) 2/6/2017 46Prof.Dr.R.R.Deshpande
- 47. Piles –Causes • 1) Standing or prolong sitting ( blood has to flow against gravity ) • 2) Defaecation - The veins passes through mucosa of anus & rectum .They get constricted if there are hard stool • 3) Excessive straining • 4) Absence of valves or congenital weak veins • 5) Pregnancy - Due to the pressure effect & hormones which relaxes muscles of the vein. • 6) Carcinoma of rectum due to backpressure. • 7) Portal Hypertension 2/6/2017 47Prof.Dr.R.R.Deshpande
- 48. Classification of Piles – Antomical Type Site of Piles Internal Hemorrhoids Situated above dentate line & covered with mucosa External Hemorrhoids situated below dentate line & covered with skin. Interno external Hemorrhoids situated above & below dentate line & covered with mucosa & skin 2/6/2017 48Prof.Dr.R.R.Deshpande
- 49. Classification of Piles – Position Type of Pile Position Primary Piles situated at --11, 7 & 3 o’clock position Secondary Piles situated at -- 1 o’clock, 2 o’clock 2/6/2017 49Prof.Dr.R.R.Deshpande
- 50. Classification of Piles – Prolapse Degree Condition of Piles First Only bleeding but do not come out of anus Second Protrude during defaecation but goes automatically inside the anus Third Protrude out & has to pushed inside manually Forth Protrude out ,not only during defaecation but even during coughing, sneezing, laughing & remains outside . 2/6/2017 50Prof.Dr.R.R.Deshpande
- 51. Piles – Clinical Features • 1) Painless Bleeding - bleeding after defecation, which is dropwise or splash in the pan. • External piles doesn’t bleed usually but gives only pain • 2) Protrusion of Mass 3) Discharge of Mucus • 4) Itching or Irritation 5) Soiling of under garments 2/6/2017 51Prof.Dr.R.R.Deshpande
- 52. Piles – P/R Examination • Internal piles can’t be felt unless they are secondary infected • Proctoscopy - Internal piles bulge into lumen of proctoscope which are in purple colour 2/6/2017 52Prof.Dr.R.R.Deshpande
- 53. Grades of Piles 2/6/2017 53Prof.Dr.R.R.Deshpande
- 55. Piles – Complications • Pain – when there is secondary infection. • Thrombosis • Ulceration • Suppuration 2/6/2017 55Prof.Dr.R.R.Deshpande
- 56. Piles – Medical Treatment • Purgatives. • Sitz bath • Local -- Xylocaine Jelly if pain. • Tab Voveron LA – 1 BD. • Antibiotics --- if infection is suspected • Laxatives – To avoid straining 2/6/2017 56Prof.Dr.R.R.Deshpande
- 57. Piles – Surgical Treatment • Lord’s dilatation • Injection therapy • Baroon band ligation • Cryo surgery • Infra Red coagulation • Transfix & ligation • Hemorrhoidectomy • Ksharsutra therapy 2/6/2017 57Prof.Dr.R.R.Deshpande
- 58. Dry Piles • (i) Kankayan Guti -- 2 Tab. 3 times a day • (ii) Triphala Guggulu ---- 2 Tab. 3 times a day • (iii) Abhayarishtha -- 4 tablespoon with equal amount of water 2 times after meals. 2/6/2017 58Prof.Dr.R.R.Deshpande
- 59. Dry Piles • (i) Kutaja Ghana vati -- 2 Tab. 3 times a day • (ii) Arogyavardhini -- 2 Tab. 3 times a day • (iii) Amrutbhallatakavleha -- 1 tablespoon each morning • (iv) Gandharva Haritaki Churna -- 1 tablespoon at bed time with warm water. 2/6/2017 59Prof.Dr.R.R.Deshpande
- 60. Dry Piles – Locally • (i) Apply Sarjarasa malahar or Shatadhout ghruta locally • (ii) Fumigate with Guggulu, Vacha, Dhoopa, Owa etc. • (iii) Apply Chukra Taila and advice Sit’z bath. 2/6/2017 60Prof.Dr.R.R.Deshpande
- 61. Bleeding Piles • (i) Bolabaddha Rasa -- 2 Tab. 3 times a day • (ii) Samasharkara Churna -- 2 Tsf 3 times a day • (iii) Triphala Churna -- 2 tablespoon at bed time with ghee and warm water 2/6/2017 61Prof.Dr.R.R.Deshpande
- 62. Bleeding Piles • (i) Praval Vati (HP) -- 2 Tab. 3 times a day • (ii) Kamaduha Vati (HP)-- 2 Tab. 3 times a day • (iii) Kutajarishtha --4 tablespoon with equal amount of water times after meals. 2/6/2017 62Prof.Dr.R.R.Deshpande
- 63. Bleeding Piles • (i) Pilex (Himalaya) -- 2 Tab. 3 times a day. • (ii) Pyroids (B) 2 Tab.-- 3 times a day. • OR • (i) Arshonyl (C) --2 Tab. 3 times a day. • OR • (i) Nagkeshar Churna – 1 table spoon with butter and warm water 3 times a day. 2/6/2017 63Prof.Dr.R.R.Deshpande
- 64. Bleeding Piles • Local Application :----- • (i) Shatadhouta Ghruta • (ii) Pilex, Arshonyl ointment. 2/6/2017 64Prof.Dr.R.R.Deshpande
- 65. Bleeding Piles-Regimen • (i) Use of Suran (only for Dry piles) and Takra (butter milk) is advisable. If excessive bleeding, instead of Suran, take black resins 30 to 40 each day. • (ii) Old rice, wheat, Takra, Shunth (dry ginger powder), Padaval etc. are good for piles. 2/6/2017 65Prof.Dr.R.R.Deshpande
- 66. Bleeding Piles -Regimen • (iii) Stay away from spicy, hot food and curd. • (iv) Sitting on uneven surface, or in the same position for long, riding a bike, travelling, forcible bowel movements are to be avoided. 2/6/2017 66Prof.Dr.R.R.Deshpande
- 67. Fissure in Ano • Longitudinal ulcer in the lower end of anal canal • Mostly due to constipation • Most painful condition in the anal region • Seen in young adults 2/6/2017 67Prof.Dr.R.R.Deshpande
- 68. Fissure –Common site • In males is 90% at the posterior & 10% at the anterior site • In females during pregnancy due to tear of perineum resulting in loose support to the anterior anus – So common site is anterior 60% & 40% at posterior site. 2/6/2017 68Prof.Dr.R.R.Deshpande
- 69. Types of Fissure in Ano • 1) Primary --- fissure is situated at midline of anus • 2) Secondary -- situated other than midline of anus • Seen in secondary diseases like ulcerative colitis, Crohn’s disease, malignancy, syphilis, diabetes mellitus & trauma. 2/6/2017 69Prof.Dr.R.R.Deshpande
- 70. Fissure in Ano –Clinical features • 1) Pain -- Remain after defecation constant up to 4 hrs ( burning or cutting in nature) • 2) Hard stool -- pellet like • 3 )Sentinel piles -- Always present in fissure in ano. They are due to mal union, fibrosis of fissure & chronicity 2/6/2017 70Prof.Dr.R.R.Deshpande
- 71. Fissure in Ano –Clinical features • 4 )Bleeding -- Negligible in fissure .Bleeding is streak like on stool matter on a toilet paper. Sometimes as a drop. • 5 )Abscess -- Due to injury to anal gland, infection results in pus formation. • 6 ) Itching -- Due to continuous watery discharge from fissure, perianal area remains wet .This results in irritation or itching in perianal region 2/6/2017 71Prof.Dr.R.R.Deshpande
- 72. Fissure in Ano • On Inspection of Anal region -- fissure is visible in midline. • P/R Digital examination – is difficult In acute condition ,due to pain • In chronic condition -- fissure is palpable & tenderness & spasm of sphincter can be noted 2/6/2017 72Prof.Dr.R.R.Deshpande
- 73. Fissure in Ano – Medical Treatment • Locally -- Xylocaine jelly for local pain relief • Laxatives • Sitz bath • NSAIDs ,Antibiotic • Inferior haemorrhoidale nerve block may be tried for relief of pain. 2/6/2017 73Prof.Dr.R.R.Deshpande
- 74. Fissure in Ano – Surgical Treatment • Lord’s Dilatation • Fissurectomy • Sphincterectomy 2/6/2017 74Prof.Dr.R.R.Deshpande
- 75. Stretching of Anal canal • Lords procedure of anal dilatation is the easiest method to dilate the sphincter of anal canal under general or spinal anaesthesia • Patient in a Lithotomy position • There may be some faecal incontinence for a few days 2/6/2017 75Prof.Dr.R.R.Deshpande
- 76. Fissurectomy • A triangular incision (v shaped) is made with a surgical knife, starting from anal margin on each site of the fissure • Edges of fissure sutured with 2-0 chromic catgut with interrupted suture • Complication --- Anal stricture 2/6/2017 76Prof.Dr.R.R.Deshpande
- 77. Anorectal fissure • (i) Chandrakala Rasa 2 Tab. 3 times a day. • (ii) Mauktika Kamadudha 1- 2 Tab. 3 times a day. • (iii) Abhayarishtha 4 tablespoon with equal amount of water 2 times after meals • Local Application : • (i) Shatadhouta Ghruta/ Kailas Jeevan • (ii) Jatyadi Ghruta/Taila • It is always better to consult a specialist if no improvement is noted 2/6/2017 77Prof.Dr.R.R.Deshpande
- 78. Advice for Ano Rectal diseases • 1) Avoid Constipation • 2) Avoid Straining in toilet • 3) Avoid chilly, spicy, non vegetarian • 4) Avoid prolonged sitting, standing & walking 2/6/2017 78Prof.Dr.R.R.Deshpande
- 79. Advice for Ano Rectal diseases • 5) Keep Anorectal part clean & dry. This area should be washed with diluted anti septic solution like savlon or KMnO4 (sitz bath) • 6) Take a lot of liquids & butter milk. • 7) Eat fruits like Grapes, Figs & Green leafy vegetables which will help for easy evacuation of stools 2/6/2017 79Prof.Dr.R.R.Deshpande
- 80. Fistula - in - Ano • Fistula = Pipe or Tube • Abnormal communication of unhealthy granulation tissue between anal canal or rectum with external perianal skin 2/6/2017 80Prof.Dr.R.R.Deshpande
- 81. Fistula - in – Ano –Types • 1) Internal fistula • 2) External fistula 2/6/2017 81Prof.Dr.R.R.Deshpande
- 82. Fistula - in – Ano – Causes • 1)Due to persistent anal gland infection which results in ano rectal abscess, rupture inside or outside resulting in fistula • 2) Tuberculosis • 3) Ulcerative colitis • 4) Crohn’s disease • 5) Carcinoma of Rectum • 6) Diabetes mellitus 2/6/2017 82Prof.Dr.R.R.Deshpande
- 83. Fistula - in – Ano- Classification 1 • 1) Low anal fistula - Internal opening below the ano rectal ring • 2) High anal fistula - Internal opening above ano rectal ring 2/6/2017 83Prof.Dr.R.R.Deshpande
- 84. High & Low level Fistula 2/6/2017 84Prof.Dr.R.R.Deshpande
- 85. Fistula - in – Ano- Classification 2 • 1) Sub cutaneous • 2) Sub mucosal • 3) Pelvic rectal 2/6/2017 85Prof.Dr.R.R.Deshpande
- 86. Goodsall’s Rule (1900) • 1) If the external opening is anterior to an imaginary line within 3.75 cm from mid point of the anus then ----- • The fistula runs straight (directly) into the anal canal. 2/6/2017 86Prof.Dr.R.R.Deshpande
- 87. Goodsall’s Rule (1900) • 2) If the external opening is situated posterior to that line then ----- • The track usually will curve & internal opening will be on the midline posterior of the anal canal (6 o’clock). 2/6/2017 87Prof.Dr.R.R.Deshpande
- 88. Goodsall’s Rule (1900) • 3) When external opening is anterior but situated more than 3.75 cm away from anus, then --- • Track will curve & end in midline posterior in anus. 2/6/2017 88Prof.Dr.R.R.Deshpande
- 89. Fistula in Ano Types of Fistula Goodsoll’s law 2/6/2017 89Prof.Dr.R.R.Deshpande
- 90. Fistula in Ano –Clinical Features • Persistent, purulent, thick discharge, which keeps the part, always wet • Pus discharge stained with blood • Intermittent pain with relation to discharge • Internal opening felt as a buttonhole on digital examination 2/6/2017 90Prof.Dr.R.R.Deshpande
- 91. Types of Fistula • External Blind Fistula - External opening present but internal opening is absent • Internal Blind Fistula - Internal opening present but external opening is blind or absent. 2/6/2017 91Prof.Dr.R.R.Deshpande
- 92. Examination of Fistula • Inspection of peri anal region -- External opening is visible • Direction of anus is palpable towards anus or rectum. • Probing - It is carried out to see weather internal opening is complete or external opening is complete. • Methylene Blue dye is used 2/6/2017 92Prof.Dr.R.R.Deshpande
- 93. Treatment of Fistula in Ano • In acute stage antibiotic should be given after pus culture & sensitivity test, • Warm Sitz’s bath • Laxative & NSAIDs are given like Tab Combiflam or Voveron LA 100 mg BD • Surgical -- Injection therapy or Fistulotomy or Fistulectomy 2/6/2017 93Prof.Dr.R.R.Deshpande
- 94. Benefits of Ayurvedic Kshar Sutra • 1) Minimum trauma • 2) No tissue loss • 3) No incontinence ( So specially useful in High level Fistula) • 4) Cost is less • 5) It cuts & heals from the base ( Like Chemical Cautery) • 6) Very narrow & fine scar 2/6/2017 94Prof.Dr.R.R.Deshpande
- 95. Ksharsutra For Fistula 2/6/2017 95Prof.Dr.R.R.Deshpande
- 96. Benefits of Ayurvedic Kshar Sutra • 7) No bleeding or minimum bleeding occurs • 8) Low quality anesthesia is required • 9) Minimal hospital stay • 10) Recurrence rate is very low 2/6/2017 96Prof.Dr.R.R.Deshpande
- 97. Prolapse of Rectum • Protrusion of a mucus membrane or wall of rectum outside the anal verge is known as prolapse of rectum or Procidentia • Common in children & old persons 2/6/2017 97Prof.Dr.R.R.Deshpande
- 98. Partial Prolapse • The prolapse in which protrusion is less than 5 cm outside the anal verge is known as partial or mucosal prolapse. 2/6/2017 98Prof.Dr.R.R.Deshpande
- 99. Partial Prolapse-Causes • It may be due to undeveloped sacral curvature • Constipation. • Mostly seen after an episode of whooping cough or after acute attack of diarrhoea • Loss of fat in ischio-rectal fossa, which support to Rectum • Due to delivery trauma or tear of perineum. • Treatment -- Digital Reposition 2/6/2017 99Prof.Dr.R.R.Deshpande
- 100. Complete Prolapse • Protrusion of rectum more than 5 cm or rectal wall outside the anal verge • Seen in females associated with uterus prolapse 2/6/2017 100Prof.Dr.R.R.Deshpande
- 101. Complete Prolapse – Causes • As age advances muscles become weak due to degeneration & results in prolapse of rectum • Straining due to habitual constipation • Mostly this type of prolapse is associated with blood & mucus discharge 2/6/2017 101Prof.Dr.R.R.Deshpande
- 102. Complete Prolapse – Treatment • Thiersch’s wiring • Rectopexy • Well’s operation • Goodsall's ligature 2/6/2017 102Prof.Dr.R.R.Deshpande
- 103. Rectal Prolapse • (i) Insert prolapsed rectum inside • (ii) Use Chukra Oil / Mushaka Oil for lubrication • (iii) Make a tight bandage with above said oils over the rectum 2/6/2017 103Prof.Dr.R.R.Deshpande
- 105. Rectal Prolapse • Note : Find out the cause, more often is loose motions . treat the disease properly. • (i) Do not force yourself for evacuating the bowels. • (ii) Do not suppress natural urges like Micturition or passing the stools. 2/6/2017 105Prof.Dr.R.R.Deshpande
- 106. Pilonidal Sinus • Pilus = Hairs & Nidus = Nest • Nest of hairs into skin in the inflammatory skin known as Pilonidal Sinus • Also known as ‘Jeep Bottom Disease – Because it was more common in Jeep Drivers at the time of II nd World War. • Common in hairy person at the age of puberty. 2/6/2017 106Prof.Dr.R.R.Deshpande
- 107. Pilonidal Sinus • In western countries most commonly seen in toilet paper users • Sinus is related to subcutaneous tissue & rarely reaches to the bone & it is not related to anus 2/6/2017 107Prof.Dr.R.R.Deshpande
- 108. Pilonidal Sinus • Sinus has one or more openings • Typically projecting hairs from its mouth – This is a cardinal sign of pilonidal sinus. • Clinical features -- painful swelling, tenderness, continuous discharge • High recurrence. • Sinogram confirms the diagnosis • Treatment -- excision of sinus with bunch of hairs • Healing occurs by secondary intension. 2/6/2017 108Prof.Dr.R.R.Deshpande
- 110. Stricture of Anus & Rectum • Congenital --- Narrowing of lumen occurs at level of anal membrane • Traumatic -- Injury to rectum during sphincterectomy ,hemorrhoidectomy, excision of polyp. 2/6/2017 110Prof.Dr.R.R.Deshpande
- 111. Stricture of Anus & Rectum • Inflammation --- which may be due to -- • Tuberculosis • Ulcer • Ulcerative colitis • Crohn’s disease • syphilitic ulcer • These causes --- stricture during healing process of ulcer 2/6/2017 111Prof.Dr.R.R.Deshpande
- 112. Stricture of Anus & Rectum • Neoplastic --- Annular & ulcerative carcinoma • Miscellaneous --- Persistent internal sphincter contracture due to constipation. 2/6/2017 112Prof.Dr.R.R.Deshpande
- 113. Stricture of Anus & Rectum –Treatment • Surgical treatment is unsatisfactory So better try to prevent stricture formation • Patients are advised for -- frequent digital dilatation or anal dilator, after anus & rectum operations during healing process 2/6/2017 113Prof.Dr.R.R.Deshpande
- 114. Condyloma (Genital Warts) • Causative organism is HPV (Human Papilloma Virus) • Transmission is usually sexual who practices anal intercourse or male homosexual, Syphilis, Gonorrhea, AIDS 2/6/2017 114Prof.Dr.R.R.Deshpande
- 115. Condyloma –Clinical features • The growth looks like cauliflower • Mass is pedunculated or sessile • Protrusion of mass • Located on perianal skin like penis, vulva, • vagina & cervix • Diagnosis is confirmed by Biopsy 2/6/2017 115Prof.Dr.R.R.Deshpande
- 116. Condyloma –Clinical features • Pruritus • Wetness • Discomfort • Treatment – • Local application of caustic • Local excision of condylomata 2/6/2017 116Prof.Dr.R.R.Deshpande
- 118. Carcinoma of Rectum – Predisposing Factors • Ulcerative colitis • Smoking • Alcohol • Crohn’s disease • Polyp • Fistula 2/6/2017 118Prof.Dr.R.R.Deshpande
- 119. CA Rectum – Clinical Features • Increase in constipation (early symptom) or Alternate Constipation & Diarrhoea • Painless bleeding -- maroon color (early symptom) • Sense of incomplete defecation • Tenesmus 2/6/2017 119Prof.Dr.R.R.Deshpande
- 120. CA Rectum – Clinical Features • Mucus discharge with stool • Loss of appetite & weight • Pain is last symptom • Abdomen distension due to obstruction • Metastasis signs are -- Ascites, Jaundice, Backache, enlarged lymph nodes, hemoptysis 2/6/2017 120Prof.Dr.R.R.Deshpande
- 121. CA Rectum– Examination • P/R Examination -- should be done in every case of PR bleeding • An indurated growth or ulcer can be felt • After removing of finger it is stained with blood • Proctoscopy - Bleeding ulcer or growth may be visible. • Colonoscopy • Biopsy 2/6/2017 121Prof.Dr.R.R.Deshpande
- 123. CA Rectum - Duke’s Classification • a) Marking ‘A’ - Growth is involved in rectum & anus • b) Mark ‘B’ - Growth beyond rectal wall but lymph nodes aren’t enlarged • c) Mark ‘C’ - Lymph nodes are enlarged • C1 – Local & C2 - In course of circulation. • Treatment -- Permanent Colostomy 2/6/2017 123Prof.Dr.R.R.Deshpande
- 124. Bleeding per rectum-Causes • Congenital - Rectal polyp • Traumatic - Injury to rectum or anus • Fissure in Ano ( Severe pain with bleeding) • Bleeding Piles ( Dropwise or splash of bleeding) • Fistula in Ano ( Blood with mucus) 2/6/2017 124Prof.Dr.R.R.Deshpande
- 125. Bleeding per rectum-Causes • Inflammatory – • Dysentery • Crohn’s Disease • Ulcerative colitis • Tuberculine ulcer in intestine 2/6/2017 125Prof.Dr.R.R.Deshpande
- 126. Bleeding per rectum-Causes • Neoplastic – • Tumor of intestine • Carcinoma of colon or rectum or anus • Miscellaneous - Piles Prolapse Fistula • Drugs Group 1) Anti-coagulant 2) Endo Methacin 3) Chloroquine 4) Aspirin 5) Cortico- steroids 6) Phenyl Butazone 2/6/2017 126Prof.Dr.R.R.Deshpande
- 127. Bleeding per rectum • For any kind of per rectal bleeding use following symptomatic treatment • Chandrakala Rasa 50 mg. + Praval Bhasma 50 mg. + Mauktika Bhasma 50 mg. + Amalaki Churna 500 mg. + Nagkeshar Churna 25 mg. 3 times a day 2/6/2017 127Prof.Dr.R.R.Deshpande
- 128. Pruritus Ani with Discharge -Causes • Piles • Condylomata • Polyps • Carcinoma of anus • Any growth • Fissure • Fistula 2/6/2017 128Prof.Dr.R.R.Deshpande
- 129. Pruritus Ani with vaginal problems • Trichomonal vaginitis • Cervicitis • Leucorrhoea 2/6/2017 129Prof.Dr.R.R.Deshpande
- 130. Pruritus Ani with worms & Fungus • Threadworm • Monilial infection • Tinea cruris 2/6/2017 130Prof.Dr.R.R.Deshpande
- 131. Pruritus Ani with skin problems • Allergic dermatitis • Psoriasis • Eczema 2/6/2017 131Prof.Dr.R.R.Deshpande
- 132. Pruritus Ani with Metabolic problems •Obstructive Jaundice • Diabetes mellitus 2/6/2017 132Prof.Dr.R.R.Deshpande
- 133. Pruritus Ani –Other causes • Excess or frequent use of laxative drugs -- causes excessive secretions • Synthetic or rough inner garments • Poor hygiene of perianal region. 2/6/2017 133Prof.Dr.R.R.Deshpande
- 134. Anal Itching –Summary • Itchy skin around anus • Causes – • Skin diseases like scabies ,Tinea • Allegic reactions to under garments • Uncontrolled DM • Fissure ,Fistula in ano ,Thread worms • Liver diseases • Cancer 2/6/2017 134Prof.Dr.R.R.Deshpande
- 135. Anal Itching –Ayurved Principles • Krumighna • Kandughna • Kaphaghna • Rakta prasadan 2/6/2017 135Prof.Dr.R.R.Deshpande
- 136. Ano Rectal Pain • All the anal conditions below dentate line are painful because supplied by spinal nerve segment • Conditions ,above dentate line are painless as long because they are supplied by autonomous nervous system • These painless lesion can become painful ,when they spread beyond rectal wall by inflammation & infiltration. 2/6/2017 136Prof.Dr.R.R.Deshpande
- 137. Various painful Ano Rectal conditions Sr.No Condition Cause 1 Continuous Throbbing pain Perianal or Anorectal abscess 2 Sharp cutting, burning, shooting pain Fissure in Ano 3 Pain is intermittent Chronic sinus or Fistula 4 Painless ulcer Syphilitic 5 Lower Abdomen Pain Obstructive lesion within the rectum 6 Tenesmus Rectal growth 2/6/2017 137Prof.Dr.R.R.Deshpande
- 138. Perianal haematoma • (i) Triphala Guggulu 2 Tab. 3 times a day • (ii) Gokshuradi Guggulu 2 Tab. 3 times a day • (iii) Vatavidhvans Rasa 1 Tab. 3 times a day • (iv) For local application . Dashang Lepa 2/6/2017 138Prof.Dr.R.R.Deshpande
- 139. Abscess (Peri anal) • (i) Sukshma Triphala (AYR) 2 Tab. 3 times a day. • (ii) Gandhak Rasayana 2 Tab. 3 times a day. • (iii) Septilin 2 Tab. 3 times a day. • (iv) Triphala Guggulu 2 Tab. 3 times a day. • (v) Local application : Lepa Goli • Note : With the treatment, if there is pus in the absess incision and drainage is a better choice, if no facility refer to a specialist. 2/6/2017 139Prof.Dr.R.R.Deshpande
- 140. Anal incontinence • Anal incontinence is defined as loss on control of defecation act • Anorectal ring is the important structure to control defaecation act • Anorectal ring marks the junction between the rectum & anal canal • It is formed by pubo rectalis, highest part of internal sphincter, longitudinal muscle & external part of sphincter 2/6/2017 140Prof.Dr.R.R.Deshpande
- 141. Anal incontinence –Causes • 1) Traumatic to rectum & anal canal • 2) Surgical procedure of rectum & anal canal • 3) Neurological causes • 4) Malignancy 2/6/2017 141Prof.Dr.R.R.Deshpande
- 142. Anal incontinence –Causes • 5) Congenital anomalies • 6) Old age • 7) Malnutrition • 8) Rectal prolapse or prolapsed piles 2/6/2017 142Prof.Dr.R.R.Deshpande
- 143. Anal incontinence –Causes • 9) Diarrhoea • 10) Irritable bowel syndrome ( IBS) • 11) Psychological 2/6/2017 143Prof.Dr.R.R.Deshpande
- 144. Anal incontinence –Treatment • Temporary incontinence – Reassurance & perineal exercises to improve the tone of internal & external sphincter. • Suturing of the torn sphincter • Permanent incontinence – inter sphincteric repair of puborectalis & plication of the external sphincter 2/6/2017 144Prof.Dr.R.R.Deshpande
- 145. Proctitis • Inflammation of rectal mucosa with inflammation of colon & anal canal • Types – • Acute or chronic • non specific or specific 2/6/2017 145Prof.Dr.R.R.Deshpande
- 146. Proctitis –Causes • Bacillary dysentery • Amoebic proctitis • Gonococcal • Lymphogranuloma inguinale • Tuberculosis • Enema - Complication 2/6/2017 146Prof.Dr.R.R.Deshpande
- 147. Proctitis –Clinical Features • Pain • Tenesmus • Mucus & pus discharge • Frequent urge to pass stool • Local Tenderness 2/6/2017 147Prof.Dr.R.R.Deshpande
- 148. Proctitis - Investigations • Proctoscopy • sigmoidoscopy • stool culture • Biopsy 2/6/2017 148Prof.Dr.R.R.Deshpande
- 150. Proctitis • Treat the root cause • Antibiotics • Anti amoebic • Retention enema of prednisolone • Tab salazopyrin 2/6/2017 150Prof.Dr.R.R.Deshpande
- 151. Rectal polyp • Any circumscribed mass of tissue that arises from mucosa & protrudes into the lumen of rectum • Common in children in the first decade of life • May appear in adults also • Rare after 30 years of age 2/6/2017 151Prof.Dr.R.R.Deshpande
- 152. Rectal polyp –Causes • Congenital • Inflammatory • Neoplastic • Miscellaneous 2/6/2017 152Prof.Dr.R.R.Deshpande
- 153. Rectal polyp –Clinical Features • Streaks of blood on the stool or sometimes profuse bleeding • Protrusion of mass during defecation • Mucous discharge • Anaemia due to recurrent bleeding • Tenesmus • Usually it is painless but painful if infected 2/6/2017 153Prof.Dr.R.R.Deshpande
- 154. Rectal polyp –Examination • P/R Examination • Proctoscopy • Sigmoidoscopy 2/6/2017 154Prof.Dr.R.R.Deshpande
- 155. Rectal polyp –Treatment • Excision – polypectomy 2/6/2017 155Prof.Dr.R.R.Deshpande
- 156. Ayurved & Guda Bhransha ( Rectal Prolapse ) • Acute & Chronic • Concern diseases – Arsha ,Malavrodha,Bhagandar • Dosha –Vata ,Dhatu – Mansa ,Mala –Purisha • Srotas – Anna, Purisha,Mutra ,Mansavaha • Chikitsa – Vatanuloman, Vata shaman, Deepan,Pachan ,Langhan ,Mansa Rasayan ;Bahya – Snehan, Dhoopan 2/6/2017 156Prof.Dr.R.R.Deshpande
- 157. Ayurved & Guda Bhransha • Arogyavardhini + Triphala Guggulu – 3 each BD with Abhayarishta 4 tsf BD with equal quantity of water --- If Constipation + Erand haritaki churna 1 tsf HS + If Krumi ,add Kapiladi vati 3 tab HS • Externally apply Shatadhauta Ghruta • Anuvasan Basti – Karanj Tail or Shatavari tail 50 ml • Dhupan with – Ud ,Dhup,Vekhand,Owa ,Shopa 2/6/2017 157Prof.Dr.R.R.Deshpande
- 158. Ayurved & Guda Bhransha • If Ajjerna ,Aanah, Aatop – add Praval panchamrut tab 3 BD with Pippalyadi kadha or Panchakolasav 4 tsf with equal quantity of water • If Gudabhransha is due to Atisar –Give Sanjeevani tab 3 BD with Kutarishta 4 tsf with equal quanrity of water 2/6/2017 158Prof.Dr.R.R.Deshpande
- 159. Ayurved & Guda Bhransha • Rasayan – to improve Mansa Samvanan ( Tone of muscle ) – • Vishatinduk vati ( Kuchala or nux vomica) -2 tab after breakfast with Balarishta 4 tsf with equal quantity of water & Chukra tail Picchu at anal region at night with Bandage 2/6/2017 159Prof.Dr.R.R.Deshpande
- 160. Ayurved & Parikartik ( Fissure in Ano ) • Types – Vataja, Pittaj • Associated Diseases – • Daurbalya • Karshya • Pandu • Gudabhransha • Atisar • Bhagandar • Arsha 2/6/2017 160Prof.Dr.R.R.Deshpande
- 161. Ayurved &Parikartika( Fissure in Ano ) • Dosha – Vata prakop due to ruksha, khara, sukshma gun ,Pitta prakop due to Ushna ,Tikshna gun • Dhatu – Rasa Kshay,Rakta dushti ,Mansa Kshay ; Mala – Purisha • Chikitsa – Shaman, Vatanuloman, Vata shaman ,Rakta prasadan, Pitta shaman 2/6/2017 161Prof.Dr.R.R.Deshpande
- 162. Ayurved & Parikartika(Fissure in Ano) • Chikitsa – Praval pishti vati + Kamdudha – 3 tab each BD with Abhayarishta 4 tsf BD with equal water • If severe pain & burning – Tab Triphala Guggulu + Tab Kaishor Guggulu – 3 tab each BD & Mauktik bhasma 30 mg + Avipattikar churna 3 gm HS 2/6/2017 162Prof.Dr.R.R.Deshpande
- 163. Ayurved & Parikartika(Fissure in Ano) • If very hard stool – Chinchalavan tail 3 tsf BD ,before food • Externally --- Avagaha sweda with Luke warn Triphala + Shatavari + Arjun + Yastimadhu decoction in the morning & Shatavari Tail or Shatadhaut ghrut Pichu with Bandage or diaper at night • Pathya – soft diet ,eating black raisins & dry figs • Apathya – Dry ,spicy ,irritating food 2/6/2017 163Prof.Dr.R.R.Deshpande
- 164. Bhagandar ( Fistula in Ano ) • Associated diseases – Krumi, Malavrodha, Parikartika,Arsha,Kushtha,Vran ,Nadi vran • Dosha – Piita dushti ,Kapha prakop • Dhatu – Rasa or lasika ,Rakta dushti ,Mansa dushti • Mala – Purisha ,Kleda 2/6/2017 164Prof.Dr.R.R.Deshpande
- 165. Bhagandar ( Fistula in Ano ) • Chikitsa – Malanuloman ,Rakta shodhan ,Vrana shodhan, Vran ropan ,Agni vardhan, Kapha pitta shaman • Triphala Guggulu + Arogyavardhini + Praval pishti + Kamdudha –each 3 BD with Mahamanjisthadi Kadha 4 tsf with equal quantity of water 2/6/2017 165Prof.Dr.R.R.Deshpande
- 166. Bhagandar ( Fistula in Ano ) • If only oedema – Upanaha with Takankhar + wheat dough • Lasika strav – Upanah + apply Eladi tail or vran shodhan tail • If severe pain – Dhupan –with – Ud , Dhup, Vekhand ( Acoraus calamus) ,Owa ( Ajwain ) ,Shepa ( fennel) 2/6/2017 166Prof.Dr.R.R.Deshpande
- 167. Bhagandar ( Fistula in Ano ) • Best policy – Tatra Dhanvantariyanam Adhikaraha – refer to surgeon for Kshar sutra treatment ( Refer PPT of Ksharsutra by Prof.Dr.R.R.deshpande on slideshare.com ) • Rasayan – Tab Thayostanin ( Ayurved Rasashala ,Pune ) 3 in the morning with Sarivadyasav 4 tsf with equal quantity of water 2/6/2017 167Prof.Dr.R.R.Deshpande
- 168. Bhagandar ( Fistula in Ano ) • Pathya --- Soft diet ,Local Anorectal Hygiene • Apathya – Spicy & irritating food ,Synthetic or tight under garments ,Keeping late at night ,Alcohol ,Tobacco, Smoking,Non Veg food ,Prolonged sitting at one place ,sitting on very hard surface ,Excess travelling on bike 2/6/2017 168Prof.Dr.R.R.Deshpande
- 169. Arsha ( Piles ) • Types – Shushka ( Dry) ,Raktarsha ( Bleeding piles ) • Associated Diseases – Malavrodha, Gudabhransha,Agirna,Agnimadya,Grahani, Yakrut vicar • Dosha – Vata ,Kapha • Dhatu – Rakta dushti,Mansa ; Mala – Purisha 2/6/2017 169Prof.Dr.R.R.Deshpande
- 170. Arsha ( Piles ) • Chikitsa – Vatanuloman ,Rakta shodhan, Kaphagnha • Shushkarsha – Tab Arogyavardhini ,Kankayan guti ,Triphala guggulu – 3 tab each BD with Abhayarishta 4 tsf with equal quantity of water • If Oedema – Apply Sarjaras malam 2/6/2017 170Prof.Dr.R.R.Deshpande
- 171. Arsha ( Piles ) • If Pain – Upanaha with dove of Jwar or Dhupan with – Dhup,Ud,Vekhand,Owa or Avagaha sweda with Triphala ,Dashamul decoction • Raktarsha – Tab Bolbaddha ras ,Praval pishti ,Kamdudha ras – each 3 tab BD with Ashokarishta + Kutajarishta - 4 tsf each with equal quantity water 2/6/2017 171Prof.Dr.R.R.Deshpande
- 172. Raktarsha Arsha ( Piles ) • If severe weakness due to bleeding – • Mauktik Bhasma 50 mg + Nagkeshar churna 500 mg + Tapyadi loha vati 2 tab BD – with Lohasav 4 tsf with equal quantity of water • Dhupan is contraindicated 2/6/2017 172Prof.Dr.R.R.Deshpande
- 173. Arsha ( Piles ) • Pathya --- Soft diet ,Local Anorectal Hygiene • Apathya – Spicy & irritating food ,Synthetic or tight under garments ,Keeping late at night Alcohol ,Tobacco, Smoking, Non Veg food Prolonged sitting at one place ,sitting on very hard surface ,Excess travelling on bike 2/6/2017 173Prof.Dr.R.R.Deshpande
- 174. Prof. Dr.R.R.Deshpande • Sharing of Knowledge • FOR • Propagating Ayurved 2/6/2017 174Prof.Dr.R.R.Deshpande