Downloaded 181 times

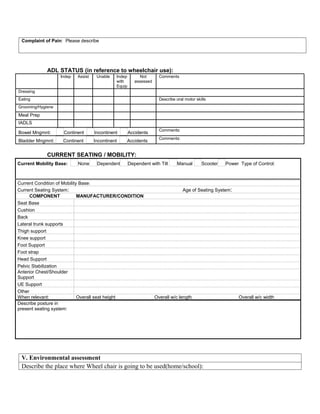
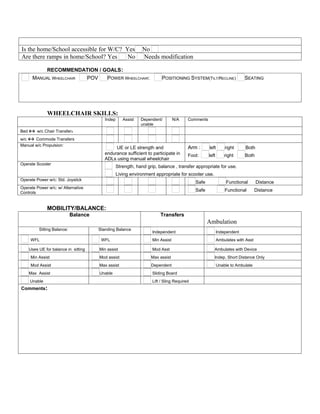
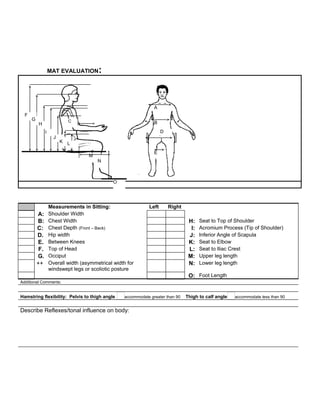

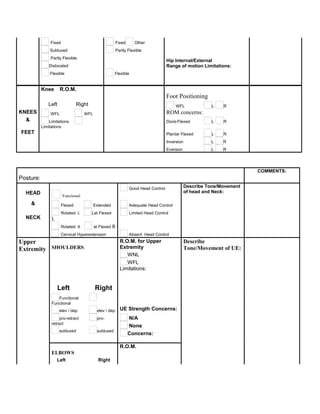
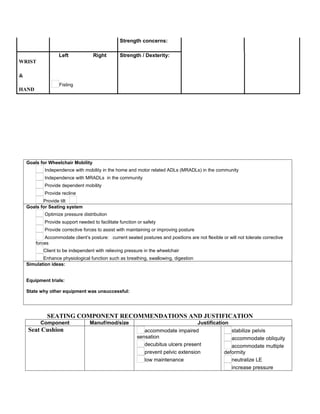




This document provides a wheelchair assessment form for collecting information about a patient's medical history, physical abilities, and needs for wheelchair seating and mobility equipment. The form collects details on diagnosis, posture, range of motion, strength, sensation, skin integrity, functional mobility, communication abilities, and environmental factors. Measurement data and photos are also included. Recommendations are made for specific wheelchair components to meet the patient's needs and facilitate independence.





















































































