3. 7/13/2023 3
•To have a basic knowledge
about Head Trauma
• To Understand the assessment
& management principles of
patients with Head Trauma
4. Definion
Head injury:- Is an injury which occurs on scalp, skull and brain
tissue
Primary brain injury
The damage caused to the brain at the moment of impact.
Concussion
Diffuse axonal injury
Contusion/laceration
Secondary brain injury
occurs at some time after the moment of impact and is often
preventable.
7/13/2023 4
5. Head injury occurs with an incidence of
20–40 cases per 100 000 population per
year.
It is the most common cause of death in
young adults(age 15–24 years)
It is more common in males than females.
7/13/2023 5
6. Road traffic accident
65% of deaths following severe head injury
Falls
Assaults
Injuries at work place, during sport, or at
home
7/13/2023 6
10. Brain metabolism
Brain oxygen consumption (CMRO2,
cerebral metabolic rate for oxygen) is
about 3.5 ml /100 g/min
The brain relies on blood borne
glucose for 90% of its energy
requirements
7/13/2023 10
11. Cerebral blood flow and autoregulation
Normal cerebral blood flow is approximately 55ml/100 g/min
MAP of brain is between 50 and 150 mmHg.
In head injury, mechanisms of cerebral authoregulation become
disordered.
Cerebral blood flow fluctuates with MAP and the brain is more
vulnerable to hypotension.
CBF=CPP/CVR , Normal CPP=60-70 mmHg
CPP=MAP-ICP, Normal ICP= 5-10mmHg
MAP = SBP + 2 DBP
3
7/13/2023 11
12. 7/13/2023 12
Monroe-Kellie doctrine
The sum of the intra cranial volumes of blood, brain,
and other components (tumor, hematoma)is
constant, and that an increase in any one of these
must be compensated by an equal decrease in
another or else pressure will rise.
13. 1. Primary & secondary
2. Glasgow Coma Score
3. Skull fracture
4. Anatomy of bleeding
5. Closed & open
6. Coup & countercoup
7. Bone involved & types
7/13/2023 13
14. Primary brain injury
The damage caused to the brain at the moment of impact.
Concussion
Diffuse axonal injury
Contusion/laceration
Secondary brain injury
Occurs at some time after the moment of impact and is
often preventable.
7/13/2023 14
16. There are three types
1. Mild head injury: GCS 14 or 15
2. Moderate head injury: GCS 9–13
3. Severe head injury: GCS 3–8
7/13/2023 16
17. 7/13/2023 17
The GCS is composed of eye (E), verbal (V) and motor (M) responses
Eyes open Spontaneously 4
To verbal command 3
To painful stimulus 2
Do not open 1
Verbal Normal oriented conversation 5
Confused 4
Inappropriate/ words only 3
Sounds only 2
No sounds 1
Motor Obeys command 6
Localize pain 5
Withdrawal/flexion 4
Abnormal flexion (decorticate) 3
Extension (DE cerebrate) 2
No motor response 1
18. A head injury may be classified according to the
type of injury that has occurred on skull.
May be divided into
- Blunt or penetrating
- Vault or basal fracture
7/13/2023 18
19. TBI in which the skull & Dura mater remain intact.
7/13/2023 19
20. When an object pierces the skull and breaches the Dura matter
Low-velocity injuries such as those caused by stabbing
High-velocity injuries such as gunshot injuries
7/13/2023 20
21. Roof of the skull
Open or closed
Linear or comminuted
Depressed or non-depressed
7/13/2023 21
24. Mild head injury
• Headache
• Confusion
• Light headedness
• Dizziness
• Blurred vision or tired eyes
• Fatigue or lethargy
• A change in sleep patterns
• Behavioral or mood changes, and
• Trouble with memory, concentration, attention,
7/13/2023 24
25. Repeated vomiting or nausea,
Convulsions or seizures,
Inability to awaken from sleep,
Dilation of one or both pupils of the eyes,
Slurred speech,
Weakness or numbness in the extremities,
Loss of coordination, and/or increased
confusion, restlessness,
7/13/2023 25
26. Leaking cerebrospinal fluid (a clear fluid drainage
from nose, mouth or ear)
Visible deformity or depression in the head or face;
Wounds or bruises on the scalp or face.
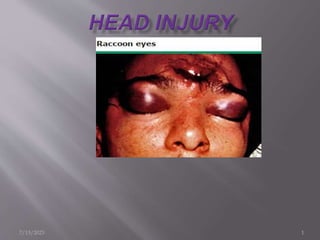
Basilar skull fractures, those that occur at the base of
the skull, are associated with
Battle's sign,(bruising over mastoid)
Hemotympanum, (or bleeding from ear)
Cerebrospinal fluid rhinorrhea and otorrhea
"halo" sign also called the "ring" or "target" sign
beta-trace protein or beta-2 transferrin
Bilateral per-orbital edema (raccoon eyes)
7/13/2023 26
27. Routine lab exam
X-Ray of head
X-Ray of cervical spines
CT-Scan – the first-line investigation
EEG
MRI
7/13/2023 27
28. 1. GCS<13 at any stage
2. GCS =13 or 14 at 2hours following injury
3. Suspected open or depressed #
4. Any sign of basal skull #
5. Post-traumatic seizures
6. Focal neurologic deficit
7. Post-traumatic amnesia of >30 minutes
8. Persistent vomiting
9. Mild head injury over the age of 65
10. On anti-Coagulants or coagulopathy
11. Significant mechanism of injury
7/13/2023 28
29. Management of head injuries
Triage well
Early discharge if the criteria met
Scalp wounds need closure
Significant depressed fractures need elevating, antibiotics
and antiepileptic
Skull base fractures may be associated with CSF leak.
Pneumococcus vaccination is valuable, but prophylactic
antibiotics are not usually indicated
7/13/2023 29
30. ABC’s of life support
Some patients with mild head injury are at
significant risk of intracranial hematoma and
require a CT scan
CT scan if fulfills the criteria if not
Discharge with Medical advice, when to return
to the emergency department.
7/13/2023 30
31. GCS 15/15 with no focal deficits
Normal CT brain if indicated
Patient not under the influence of alcohol or drugs
Patient accompanied by a responsible adult
Verbal and written head injury advice:
Seek medical attention if:
Persistent/worsening headache despite analgesia
Persistent vomiting
Drowsiness
Visual disturbance
Limb weakness or numbness
7/13/2023 31
32. The principal aim of treatment is the prevention of
secondary brain injury and this is best achieved
by the avoidance of hypoxia and hypotension.
ABC’s of life support
10-15% of head injury patients have Spine injury.
Look for any other site of injury
Other measures
Surgical management
7/13/2023 32
33. Comes after the management of life-threatening
conditions.
The goal of critical care is designed to rapidly identify,
record, treat & prevent secondary brain injury.
Occur within minutes, hours, or days after the primary
injury and can lead to further damage of nervous tissue,
contributing to permanent neurological dysfunction.
Include hypoxia, hypotension, ICP, Seizure, hyperglycemia.
7/13/2023 33
34. 1)Prophylaxis against Cushing’s (stress) ulcers seen
in STBI
antacid and/or H2 antagonist/ sucralfate / PPI
2) Aggressive control of fever (fever is a potent
stimulus to increase CBF
3) IV fluids:
Isolated head injury: the choice is isotonic (e.g. NS + 20 m Eq KCl/L)
Avoid hypotonic solutions (e.g. LR) which may impair cerebral
compliance
7/13/2023 34
35. 4)Avoid hypoxia (PaO2<60mm Hg or O2 sat <90%)
Hypoxia may cause further ischemic brain injury
Immediate goal – to maintain adequate cerebral
oxygenation
maintain airway and ventilation
5) Avoid arterial hypotension - Strongly associated with poor
prognosis
Maintain SBP>90mmhg &DBP> 60mmhg in order to keep CPP
>60mmhg
2x mortality, 3x when hypoxia + hypotension
6) Control hypertension if present
Nicardipine if not tachycardic
Beta-blocker if tachycardic (labetalol, esmolol)
7/13/2023 35
36. 7)Prevent hyperglycemia: (aggravates cerebral edema)
usually present in head injury, may be exacerbated by
steroids
8) Intubation : for GCS≤8 or respiratory distress.
Give IV lidocaine first and antibiotics
9) light sedation: codeine 30–60 mg IM q 4 hrs, or
lorazepam 1–2mg IV q 4–6 hrs
10) Head Position- Keep head of bed at 30-45◦
Enhancing venous outflow
Promoting displacement of CSF
7/13/2023 36
37. Monroe Kellie hypothesis
Normal ICP varies with age.
7/13/2023 37
38. 1.Cerebral edema
2.Hyperemia
3.Trauma ass. Masses
a. Extra-axial bleedings
b.Haemorrhagic contusion
c.Foreign body
d.Depressed Skull Fracture
4.Hypoventilation
5.Increased muscle tone and valsalva maneuver
6.Sustained posttraumatic seizures (status
epilepticus)
7/13/2023 38
39. A secondary increase in ICP is sometimes observed 3–10
days following the trauma, and may be associated with
a worse prognosis
Possible causes include:
Delayed hematoma formation
Cerebral vasospasm
Severe adult respiratory distress syndrome (ARDS)
with hypoventilation
Delayed edema formation: more common in pediatric
patient
Hyponatremia
7/13/2023 39
40. Goals of therapy
1.Keep ICP < 20mmhg
2.Keep CPP ≥70mmhg(i.e avoid hypotension)
Management Modalities
Surgical Rx
Any significant sub dural or epidural haematoma
Significant high contusions with mass effect
7/13/2023 40
41. 1) Heavy sedation and/or paralysis when necessary
MSO4: 2–4mg/hr IV drip
Fentanyl: 1–2ml IV q 1 hr (or 2–5 mcg/kg/hr IV drip)
Sufentanil: 10–30 mcg test dose, then 0.05 -2 mcg/kg/hr
IV drip
Midazolam : 2mg test dose, then 2–4mg/hr IV drip
Propofol drip: 0.5 mg/kg test dose, then 20–75
mcg/kg/min IV drip avoid high dose propofol (do not
exceed 83 mcg/kg/min)
“low dose” pentobarbital (adult: 100 mg IV q 4 hrs)
7/13/2023 41
42. 2) CSF drainage (when IVC is used): 3–5ml
3) Osmotic therapy
Mannitol=0.25–1 gm/kg bolus (over <20 min) followed by
0.25 gm/kg IVP (over 20 min) q 6 hrs
May“alternate”with: furosemide 10–20 mg IV q 6 hrs
Hypertonic saline= refractory to mannitol
continuous 3% saline in fusion or as bolus of 10–20 ml of 23.4% saline
D/C after ≈ 72 hours
Hold osmotic therapy if serum osmolarity is ≥320 mOsm/L
or SBP<100
7/13/2023 42
43. 4) Hyperventilation (HPV) to PaCO2=30–35 mmHg use only
for
Short periods for acute neurologic deterioration
Chronically for unresponsive to sedation, paralytics, CSF
drainage and osmotic therapy
Avoid HPV during the first 24 hrs after injury
7/13/2023 43
44. “Second tier” therapy for persistent ICP
Repeating a head CT to rule out a surgical condition
EEG to rule - outsubclinical status epilepticus
1)High dose barbiturate therapy : initiate if ICP
remains >20–25 mmHg
2)Hyperventilate to PaCO2=25–30 mm Hg
7/13/2023 44
45. 3) Hypothermia= reduce cerebral metabolism—dec in
CBV and ICP
6–7% ↓ CMRO2 for every 1°C decrease in
temperature
Neuroprotective-Decreases the release of excitotoxic
amino acids
Monitored for a drop in cardiac index,
thrombocytopenia, elevated creatinine clearance, and
pancreatitis
4) Decompressive surgery
7/13/2023 45
46. Early (≤ 7days) or late(>7days) after head trauma.
Early = 30% of STBI.
May precipitate adverse events as a result of ↑ of
ICP, alterations in BP, changes in oxygenation, and
excess neurotransmitter release.
Late PTS = within 2 years of head injury.
Prophylactic AEDs= only to prevent early onset
PTS.
7/13/2023 46
47. 1.Acute subdural, epidural or intracerebral
hematoma
2.Open DSF with parenchymal injury
3.Seizure within the first 24hrs after injury
4.GCS<10
5.Penetrating brain injury
6.History of significant alcohol abuse
7.Cortical hemorrhagic contusion on CT
7/13/2023 47
48. Drug of choice Phenytoin
Should be started within the first 24hrs of
injury.
AEDs must be tapered after 1 week.
Might be used for more weeks in:
Penetrating brain injury
Prior seizure history
Patients undergoing craniotomy
7/13/2023 48
49. Nutrition support must be initiated within 24-48 hrs of
admission.
Increase in energy expenditure in head injury.
A balance must be maintained between the patient’s
metabolic needs and nutrition support
The best indicator of nutritional adequacy is overall
clinical improvement.
When wounds are healing, infection is resolving, and
patients are weaning off the ventilator.
7/13/2023 49
50. STBI pts are prone to developing DVT(up to 25% ) b/c
Prolonged bed rest
Paralyzed limbs
Long operating times of some procedures.
Prophylaxis against DVT
1.General measures
Passive range of motion
Early ambulation
2.Mechanical techniques
Pneumatic compression boots
Electrical stimulation of calf muscles
Rotating beds
3.Anti coagulation=heparin
7500 iu SC BID/TID may be started at admission or immediate
post op
7/13/2023 50
51. Principles
Remove a compressive surface hematoma as
soon as possible.
Conservative approach for hemorrhagic
contusions or intra-cerebral lesions
7/13/2023 51
52. Standard burr hole sites
Frontal -8cm above the supra-ciliary ridge & 3cm from the midline
Parietal -on the parietal eminence
Temporal -1cm in front of the external auditory meatus, just above the
zygomatic arch
7/13/2023 52
54. Laceration of the artery (mostly middle
meningeal)
7/13/2023 54
55. Is a neurosurgical emergency
It results from rupture of an artery, vein or venous sinus, in association
with a skull fracture
Commonly the middle meningeal artery under the thin temporal bone
A low energy injury mechanism, with brief loss of consciousness then
with subsequent lucid interval with headache, without any neurological
deficit
Later rapid deterioration follows
There is contralateral hemiparesis, reduced conscious level and
ipsilateral pupillary dilatation, the cardinal signs of brain compression
and herniation.
7/13/2023 55
56. On CT, extradural hematomas appear as a lentiform
( ) hyper-dense lesion between skull and brain
Areas of mixed density suggest active bleeding
Mass effect may be evident, with compression of
surrounding brain and mid-line shift
Immediate evacuation in deteriorating or comatose
patients or those with large bleeds
Close observation with serial imaging in all cases
7/13/2023 56
58. Although conservative management is often left to
clinical judgment, the "Guidelines for the Surgical
Management of TBI" recommended that patients who
exhibit an EDH that is
<30 mL,
<15-mm thick, and
<5-mm midline shift, without a focal neurological deficit
GCS >8
can be treated non-operatively.
7/13/2023 58
59. Result from tearing of the bridging veins in subdural
space
7/13/2023 59
60. It is a collection of blood between the brain & Dura
It is due to injury to the cortical veins and blood gets collected in the
subdural space forming hematoma
Hematoma is extensive and diffuse
There is no lucid interval
There is severe primary brain damage
Hematoma may be of coup and countercoup type
Loss of consciousness occurs immediately after trauma and is
progressive
Convulsion is common
7/13/2023 60
61. Hematoma is extensive and diffuse
There is severe primary brain damage
Hematoma may be of coup and counter-coup
type.
Loss of consciousness occurs immediately after
trauma and is progressive.
Convulsion is common.
Features of raised ICP
50 % mortality
7/13/2023
61
62. Features of raised intracranial pressure
is obviously seen
—high BP, bradycardia, vomiting
Focal neurological deficits or
hemiparesis can occur
CT scan shows concavo-convex lesion
50 % mortality
Treatment
Antibiotics
Anticonvulsants
Mannitol
Surgical decompression
is done by craniotomy
7/13/2023 62
63. 1 Cm thick
5 mm shift
The GCS score decreases by 2 or more
Presents with fixed and dilated pupils
ICP exceeds 20 mm Hg
7/13/2023
63
/ Craniectomy + duraplasty /
64. Inside the brain tissue
Intra-ventricular
hemorrhage
Inside the brain ventricle
Common in premature infant
7/13/2023 64
65. Indications for evacuation
GCS score 6- 8
Frontal & temporal >20 ml
Parietal >50 ml
Midline shift 5mm
Cisternae compression
Posterior fossa with mass effect
7/13/2023 65
66. Penetrating injury
Superficial debridement and dural closure to prevent CSF
leak is generally recommended
prophylactic broad-spectrum antibiotics (usually a
cephalosporin) to reduce incidence of infection
Depressed fractures
increased risk of infection and seizures
Tetanus status should be determined
Prophylactic antibiotics be given for five to seven days
Anticonvulsants should also be used to reduce the risk of
seizures.
Emergent elevation is recommended if there is a dural
tear, pneumocephalus, an underlying hematoma, or a
grossly contaminated wound.
>1cm, 5 mm below the adjacent inner table, cosmetic
7/13/2023 66
presence of beta-trace protein, which is found in high concentrations in CSF, or beta-2 transferrin, which is found only in CSF, perilymph, and aqueous humor
Raumatic IC-HTN may be due any of the following (alone or in various combinations) :
1. cerebral edema
2. hyperemia: the normal response to head injury.Possibly due to vasomotor paralysis (loss of
cerebral autoregulation). May be more significant than edema in raising ICP (p.901)
3. traumatically induced masses
a) epidural hematoma
b) subdural hematoma
c) intraparenchymal hemorrhage (hemorrhagic contusion)
d) foreign body (e.g. bullet)
e) depressed skull fracture
4. hydrocephalus due to obstruction of CSF absorption or circulation
5. hypoventilation (causing hypercarbia→vasodilatation)
6. systemic hypertension (HTN)
7. venous sinus thrombosis
8. increased muscle tone and valsalva maneuver as a result of agitation or posturing→increased
intrathoracic pressure →increased jugular venous pressure →reduced venous outflow from head
9. sustained posttraumatic seizures (status epilepticus)
Asecondar y increase in ICPis sometimes obser ved 3–10 days following the trauma, and may be associated with a worse prognosis.
12
Possible causes in clude:
1. delayed hematoma formation
a) delayed epidural hematoma (p.894)
b) delayed acute subdural hematoma (p.898)
c) delayed traumatic intracerebral hemorrhage
13
(or hemorrhagic contusions) with perilesional
edema: usually in older patients, may cause sudden deterioration. May become severe
enough to require evacuation (p.892)
2. cerebral vasospasm
14
3. severe adult respiratory distress syndrome (ARDS) with hypoventilation
4. delayed edema formation: more common in pediatric patients
5. hyponatremia
treatment for IC-HTN should be initiated for ICP > 20 mm Hg
Go a ls o f t h e r a p y
1. keep ICP≤20 mm Hg (prevents“plateau waves”fr om com p r om isin g cer ebr al blood - flow (CBF)
and causing cerebral ischemia and/or brain death
2. keep CPP≥50 mm Hg.Th e p r im a r y g o a l is t o co n t r o l ICP, s im u lt a n e o u s ly, CPP s h o u ld s u p p o r t e d by maintaining adequate MAP
Gives room for the normal brain.
Removes region of disrupted BBB
The timing of prophylaxis against deep venous thrombosis (DVT) has been an issue of controversy. There is general agreement on the need for prophylaxis, because up to 25% of patients with isolated traumatic brain injury develop DVT and most clinicians will agree with its implementation 48 hours after injury. There is some evidence to suggest that immediate postoperative use of heparin prophylaxis is safe and does not confer additional risk of bleeding
The patient may then present in the subsequent lucid interval with headache, but without any neurological deficit. At this stage, the increase in the intracranial volume is not yet causing a significant rise in intracranial pressure because compensation is occurring. However, once the limits of compensation have been reached after as long as some hours (see Monro Kellie doctrine) rapid deterioration follows. There is contralateral hemiparesis, reduced conscious level and ipsilateral pupillary dilatation, the cardinal signs of brain compression and herniation. Although this classical presentation occurs in only one third of cases, it emphasises the potential for rapid avoidable secondary brain injury in patients with minimal primary injury.
Earliest surgery and evacuation is the need
5 cm vertical incision in parietal region above the zygoma
Galea is incised. Skull is opened using perforator and burr
Meninges are kept aside
Black currant jelly clot is evacuated
Bleeding vessels are cauterized – bipolar cautery
Dural hitch stitches are placed
Opposite side if needed should be evacuated
Antibiotics;
Anticonvulsants
Manitol
Analgesics
General measures – catheter; fluid therapy
Prevention post traumatic complications