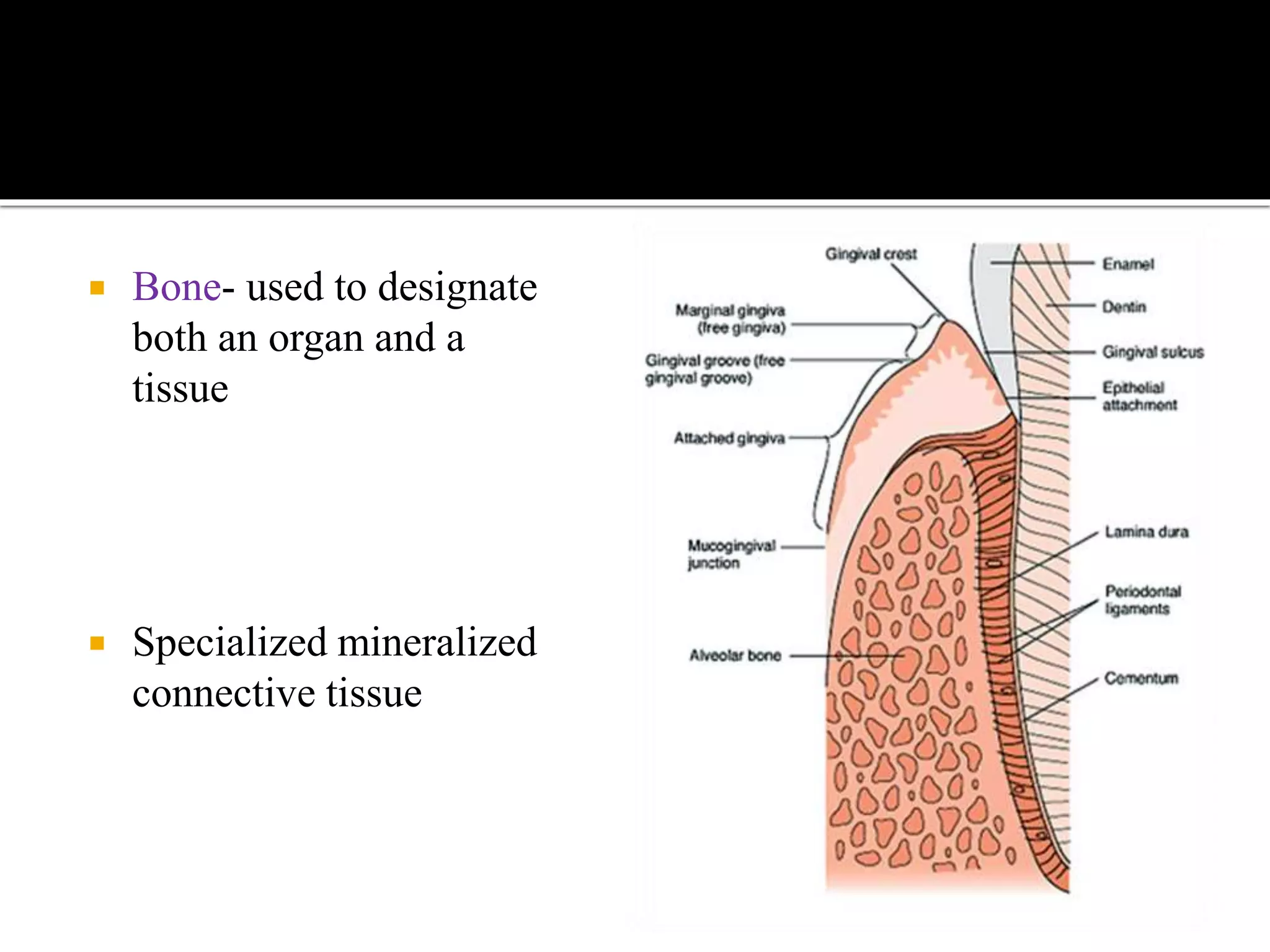
This document provides an overview of bone histology and development. It discusses that bone is a specialized mineralized connective tissue that can be divided into compact and cancellous bone microscopically. Bone develops through either endochondral or intramembranous ossification. The key cells involved are osteoblasts, which form new bone, and osteoclasts, which resorb bone. Bone is remodeled throughout life by the balanced actions of these cells.

















































































































































![ALVEOLAR BONE IN HEALTH AND DISEASE [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/alveolarboneinhealthanddiseaseautosaved-231125051936-9d7ab2b3-thumbnail.jpg?width=640&height=640&fit=bounds)

















































