

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Entamoeba by-manoj
Similar to Entamoeba by-manoj (20)
More from Manoj Mahato
More from Manoj Mahato (20)
Recently uploaded
Recently uploaded (20)
Entamoeba by-manoj
- 2. CHARACTERISTICS OF PROTOZOA 1. Protozoa are unicellular eukaryotic organism 2.Single cell perform the all the function 3.size vary from 2-150 µ 4. locomotion by pseudopodia, flagellae or cilia 5.Nucleus may be compact with diffuse central DNA and peripheral RNA. 6. Respiration anaerobic. 7.secrete digestive enzymes, toxins, cytolysin and antigenic substances. 8. Reproduction: may be asexual or sexual.
- 3. CONTENTS General character Classification Introduction Morphology Life cycle Pathogenesis Intestinal amoebiasis Clinical features Extraintestinal amoebiasis Diagnosis Treatment Prevention
- 4. GENERALCHARACTEROFENTAMOEBAHYSTOLYTICA: Unicellular, Eukaryotic Found in damp habitat Microscopic organism Single cell perform the all the function. locomotion by pseudopodia Respiration anaerobic Reproduction: may be asexual or sexual. Secrete digestive histolysin enzymes
- 6. CLASSIFICATION Phylum :- Sarcomastigophora Subphylum :- Sarcodina Superclass:-Rhizopoda Class:- Lobosea Orders:- Euamoebida Genus:- Entamoeba Species:-histolytica
- 7. INTRODUCTION Entamoeba histolytica causes amoebasis First described by Losch in 1875 after being isolated in Russia from a patient with dysenteric stool Geographical distribution World wide distribution – 3rd after malaria and schistosomiasis Worldwide amoebiasis causes 40,000-100,000 deaths every year
- 8. EPIDEMIOLOGY 0.5 to 50% of the population world wide harbors E. histolytica Higher rates of infection in underdeveloped countries. Infectaion is associated with poor hygiene. Humans are the principal host, although dogs, cats and rodents may be infected. The word histolytic literally means "Tissue destroyer“
- 9. HABITAT Large intestine of man : Trophozite Forms : Mucous and submucous layer MORPHOLOGY The parasite exists in three morphological forms: Tropozoite Precyst Cyst TROPOZOITE PRECYST CYST
- 10. Trophozite 15-30 in diameter Active, feeding stage,Growing stage Motile ,Amoeboid with blunt pseudopodia Non-infective stage Food vacuoles: RBCs, leucocytes and tissue debris Found in intestinal & extra-intestinal lesions diarrhoeal stools
- 12. PRECYST:- Smaller in size 10-20µm in diameter Oval with a blunt pseudopodium Food vacuoles disappear Characteristics nucleus
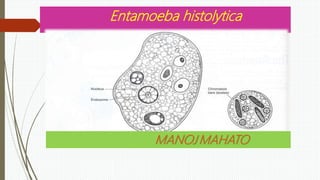
- 13. CYST Spherical, 1-15 µm in diameter Surrounded by a thick chitinous wall Uni nucleated → Bi nucleated → tetra nucleated Cyst are present only in the lumen of the colon and in formed faeces Infective form for humans Mature cyst has 4 nuclei (diagnostic feature) Not killed by chlorination Readily killed by boiling or filtration of water
- 14. Cysts of Entamoeba histolytica GHI IHG Cysts of Entamoeba histolytica /, permanent preparations stained with trichrome.
- 15. LIFE CYCLE InfectionInfection Infection occurs by ingestion of cysts on fecally contaminated food or hands.
- 16. PATHOGENESIS Ingestion of cysts Excystation in small intestine Production of 8 trophozoites Multiplication and Colonization in large intestine Tissue invasion and destruction Flask – shaped ulcers(mostly in caecum, transverse and sigmoid colon Encystation and exit from host in the stool Migrate via Blood stream( portal circulation) to the liver Amoebic liver abscess
- 17. PATHOGENICITY MODE OF TRANSMISSION: -Feco-Oral Route: By Ingestion of contaminated food and Drinking water ROUTE OF TRANSMISSION: -Fecal-oral route -By contaminated food & water Sources of infection – carriers (asymptomatic & convalescent), houseflies, cockroaches Risks – poverty, lack of hygiene, poor sanitation, mental retardation, male homosexuals INTESTINAL AMOEBIASIS : Intestinal amoebiasis indicate that organism are confined to gastrointestinal tract. Incubation period :1-4 weeks The amoebae invade the colonic mucosa , producing characteristic ulcerative flask shaped lesions and a profuse bloody diarrhea ( amoebic dysentery)
- 18. EXTRA INTESTINAL AMOEBIASIS:- About 5% individuals 1. Hepatic amoebasis: Acute Liver Abscess: Develop after 1-3 Months Transmit through portal veins from intestine to Liver Pus of liver abscess: Anchovy Sauce appearance: Contain few Pus cells liver abscess
- 19. 2. Pulmonary Amoebiasis: Transmitted from Liver and develop pulmonary Lesions 3.Cerebral Amoebiasis: Transmitted from Liver to heart then Brain and develop cerebral lesion Cerebral Amoebiasis
- 20. SIGN AND SYMPTOMS Mild symptoms include: Loose stools/diarrhoea, including slimy diarrhoea with pus (which is often foul smelling) and painful passage of stools (tenesmus) Stomach pain Stomach cramps (colic) Nausea
- 21. SIGN AND SYMPTOMS SEVERE SYMPTOMS INCLUDE: Liver abscess Severe ulceration Severe gastric distention of the bowel Peritonitis (inflammation of the intestinal wall and its lining) or colitis (inflammation of the colon, specifically) Megacolon (very rare, in 0.5% of the cases) Ameboma (which results from formation of annular colonic granulation tissue and may mimic carcinoma of the colon
- 22. LABORATORY DIAGNOSIS: Lab diagnosis is include, Parasitic diagnosis Sero diagnosis Biochemical diagnosis Radio imaging diagnosis
- 23. PARASITIC DIAGNOSIS: It includes stool examination .
- 25. STOOL EXAMINATION : (Formed stools contain cysts & diarrheal stools contain trophozoites) Wet mount in saline, Iodine-stained, or fixed trichrome stained preparation For motile trophozoites, stools should be examined within 1 hour.Trophozoite of E. histolytica is differentiated from other amoeba (E.coli) by: i. Nucleus of trophozoite For cysts, at least 3 samples should be collected. i. Size of cyst & number of its nuclei. (Newly formed cyst has 2 nuclei, glycogen mass & chromidial bars)
- 28. OBSERVATION
- 29. SERO DIAGNOSIS: Sero diagnosis by indirect heamaglutination [IHA], indirect fluorescent agglutination [IFA], [ELISA]
- 30. Radio imaging Diagnosis It’s by ultrasound CT, Scan
- 31. TREATMENT OF AMEBIASIS :- Eradication of amoeba by use of amoebicide on the basis of amoebic site
- 32. AMOEBICIDE PEDIATRIC DOSE ADULT DOSE Metronidazole 35-50 mg/kg/day for 7-10 days( in 3 divided doses) 750 mg 8 hourly Tinidazole 50 mg/kg/day for 3 days(once daily) 2 g once a day Paromomycin 25-35mg/kg/day for 7 days(in 3 divided doses) 25-35mg/kg/day (in 3 divided doses) Diloxanide furoate 20mg/kg/day for 7 days(in 3 divided doses) 500mg 8 hourly Iodoquinone 30-40mg/kg/day for 20 days(in 3 divided doses) 650mg 8 hourly DRUGS AND DOSES
- 33. PREVENTION & CONTROL Primary prevention Safe excreta disposal Safe water supply Hygiene Health education Treat symptomatic carriers Treat water Secondary Early diagnosis Treatment
- 36. COMPRISION BETWEEN AMOEBIC AND BACILLARY DYSENTERY symptoms Amoebic dysentery Bacillary dysentery Occurrence Usu. In the form of sporadic cases Usu. In the form of outbreaks Onset gradual Acute Fever Usu. Low grade (may be high in case of liver abscess) High grade Tenesmus/Abd. Cramps Moderate Very severe Stool Foul- smelling Not foul-smelling RBCs In clumps Discrete Pus cells Scanty Numerous Eosinophils Present Absent or rare Bacteria Numerous, motile Scanty, non-motile E. histolytica Trophozoites + Absent