Downloaded 410 times

![Who/What is Disordered?
“All drugs that are taken in excess have in
common direct activation of the brain reward
system…. They produce such an intense
activation of the reward system that normal
activities may be neglected. …[The] roots of
substance use disorders for some persons can
be seen in behaviors long before the onset of
actual substance use itself.” DSM-5, p. 481.](https://image.slidesharecdn.com/coredsm5-140101195744-phpapp02/85/Introduction-to-the-New-DSM-5-Manual-8-320.jpg)
![DSM-IV-TR: Categorical Method
• “The naming of categories is the traditional
method of organizing and transmitting
information in everyday life and has been the
fundamental approach used in all systems of
medical diagnosis.” p. xxxi
• “…[I]t is possible that the increasing research
on, and familiarity with, dimensional systems
may eventually result in their greater acceptance
both as a method of conveying clinical
information and as a research tool.” p. xxxii](https://image.slidesharecdn.com/coredsm5-140101195744-phpapp02/85/Introduction-to-the-New-DSM-5-Manual-23-320.jpg)
![DSM-5: A Dimensional Approach To
Diagnosis Begins
• “…[T]he once plausible goal of identifying
homogeneous populations for treatment and
research resulted in narrow diagnostic
categories that did not capture clinical
reality…. The historical aspiration of achieving
diagnostic homogeneity by progressive
subtyping with disorder categories no longer
is sensible….” DSM-5, p. 12](https://image.slidesharecdn.com/coredsm5-140101195744-phpapp02/85/Introduction-to-the-New-DSM-5-Manual-26-320.jpg)

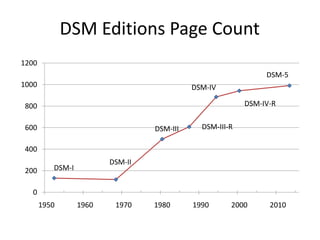
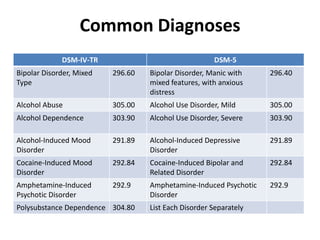
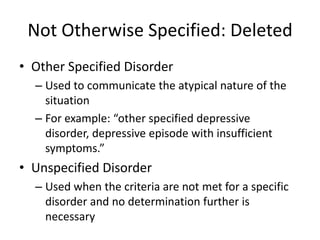
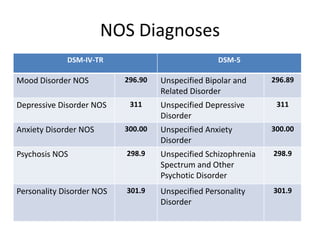
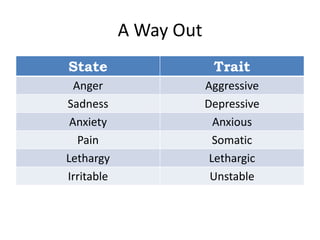
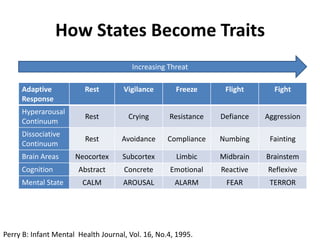
The document discusses key changes and concepts in the DSM-5, including the removal of multiaxial systems and the introduction of a dimensional approach to diagnosis. It outlines modifications in disorder classifications, such as schizophrenia, bipolar, and substance use disorders, with a focus on improving diagnostic reliability and validity. Additionally, the document highlights the transition considerations to ICD-10 and provides resources for further information on DSM-5 topics.
























![Psychodiagnostic technique[1]](https://cdn.slidesharecdn.com/ss_thumbnails/psychodiagnostictechnique1-191031121907-thumbnail.jpg?width=640&height=640&fit=bounds)