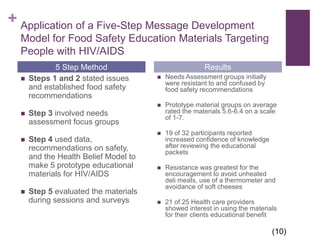
The document discusses obstacles to adequate nutrition in HIV patients. It identifies factors that compromise the immune system in HIV patients like the virus's effect on CD4 cells. Common nutrition issues in this population include malabsorption, opportunistic infections, medication side effects, and difficulty maintaining weight. The document examines methods of assessing and monitoring nutritional status in HIV patients, including medical tests, dietary recalls, and physical exams. It also outlines nutrition interventions and education needed to help HIV patients maintain adequate nutrition.

























































![HUMAN_IMMUNODEFICIENCY_VIRUS[1]. pptx](https://cdn.slidesharecdn.com/ss_thumbnails/humanimmunodeficiencyvirus1-250922103632-2012e6ee-thumbnail.jpg?width=640&height=640&fit=bounds)






