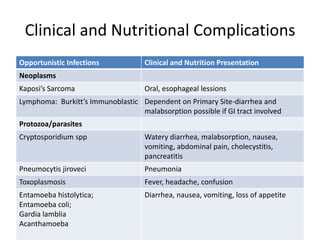
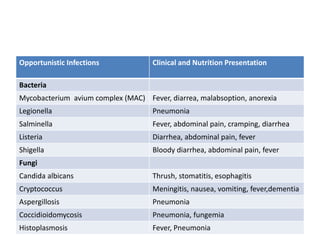
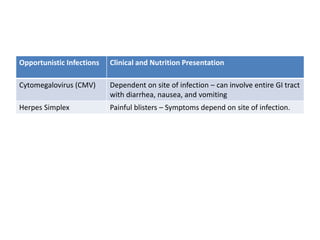
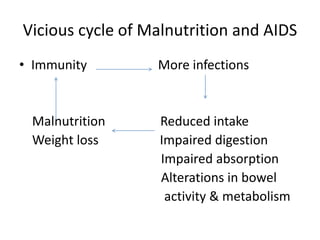
The document discusses nutrition in HIV/AIDS, covering topics such as how HIV infects cells and depletes the immune system, common opportunistic infections seen in AIDS patients, nutritional complications that can arise, causes of malnutrition, nutrition assessment, nutrition therapy goals and interventions, food safety recommendations, and the need for a multidisciplinary approach to care.