Thoracic outlet syndrome
•Download as PPTX, PDF•
28 likes•13,114 views

7th september 2015- college Activity

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Thoracic outlet syndrome
Similar to Thoracic outlet syndrome (20)
Recently uploaded
Recently uploaded (20)
Thoracic outlet syndrome
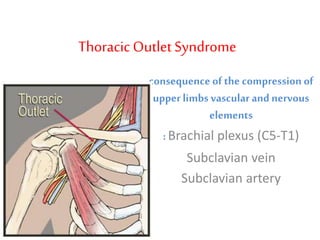
- 1. ThoracicOutlet Syndrome consequence of the compression of upper limbs vascular and nervous elements : Brachial plexus (C5-T1) Subclavian vein Subclavian artery
- 4. ANATOMY outlet is composed of 5 successive spaces the vascular and nervous elements go through : • The intercosto scalenic defile • Theprescalenic defile • Thecostoclavicular space • The sub-pectoral tunnel • The humeralspace
- 7. Costo-clavicular space • Ant : clavicle, subclavius muscle • Post medial: 1st rib • Post lateral: superior border of scapula
- 9. contents viscera • thymus • trachea • oesophagus • lung apices vessels, nervesand lymphatics • common carotid arteries • confluences of internal jugular and subclavian veins • phrenic nerves • vagus nerves • recurrent laryngeal nerves • thoracic duct prevertebral fascia muscles • sternocleidomastoid muscle • anterior and middle scalene muscles • sternohyoid muscle • sternothyroid muscle
- 11. Causes • Cervical rib • Long C7 transverse process • Anomalous insertion of scalene muscles • Scalene muscle hypertrophy • Scaleneus minimus • Abnormal bands, ligaments • Fracture clavicle/ 1st rib • Exostosis • Tumours • Brachial plexus trauma / diseases
- 13. Anatomicalabnormalities 1- Ossseous congenital abnormalities Subnumerous cervical ribs 2- C7 apophysis hypertrophy 3- rib agenesy 4- Clavicle congenital abnormalities
- 15. cervical ribs
- 16. 5- Osseous post traumatic abnormalities • Clavicle • First rib 6- Muscular and/or ligamentary abnormalities 7- Difficult to reveal preoperatively
- 17. RiskFactors • occupations that involve heavy usage of the upper extremities against resistance, including jack-hammer operators and dental hygienists, • weight lifting, • pregnancy, and obesity. • Any condition that causes encroachment of the space for the brachial plexus at the thoracic outlet can lead to thoracic outlet
- 18. Signs and symptoms of T.O.S 1-Neurologic compression • Pain and/or parasthesia of the neck, shoulder region, arm or hand, depending on the root involved • Often bilateral • Difficulty with fine motor tasks of the hand • Examination reveals : • sensitive disorders • muscle weakness • muscle atrophy (long fingers flexors) • Palpation of subclavicular area may cause pain
- 19. 2-Arterial compression : • Easily Fatigue • Weakness • Coldness • Upper limb claudication • Thrombosis • Paraesthesia • Gangrene • Raynaud's phenomenon due to thrombosis with distal embolisation • Ischemic signs, distal gangrene due to repeated embolization, or to subclavian artery thrombosis
- 21. 3-Venous compression • edema • Collateral formation • Superficial vein distension • Cyanosis • Paget-Schroetter syndrome – effort thrombosis "Effort" axillary-subclavian vein thrombosis (Paget-Schroetter syndrome) is an uncommon deep venous thrombosis due to repetitive activity of the upper limbs
- 22. Diagnosis I. History: • Neck trauma preceding onset of symptoms • Repetitive stress injury • Occipital headaches • Pain over trapezius, neck, shoulder, chest • Specific disabilities regarding work and daily activities • Exertional arm pain I. Physical Exam: • Pulse exam • Listen for bruits • Edema/cyanosis/collateral veins • Tenderness over scalene muscles (trigger points) or pectoralis minor • Reduced sensation to very light touch in fingers
- 23. ClinicalEXAMINATION diagnostictests are used to reproduce the compression and T.O.S. familiar symptoms 1- ‘‘Hands up’’ test ( Roos test) this position, the patient opens and closes his hands repeatedly : a positive test reproduces pain, heaviness or arm weakness within the first minute after beginning.
- 24. Position of thearms fortheRoos test
- 25. 2- ADSON or scalene maneuver patient rotates his head towards the tested arm while the examiner extends the arm
- 26. 3. Halsted's costoclavicular compression test • 45° abduction and extension of arm with downward pressure on shoulders –neck turned to opposite side- reproduce symptoms
- 27. 4.Exaggerated military position • shrugs shoulders with deep inhalation while drawing the shoulders backward in an exaggerated military position – radial pulse diminishes. 5.Tinel sign – in supra and infraclavicular region 6.Phalens sign – in carpel tunnel syndrome
- 28. Hyperabduction syndrome7.Wright's hyperabduction test • Arm hyperabducted to 180° diminishing radial pulse. • Neurovascular structures compressed in subcoracoid region by pectoralis minor tendon, head of humerus or coracoid process
- 29. Investigations Imaging 1. Standard X-Ray neck and thoracic examination looking for osseous abnormalities 2. MRI, cervical myelography r/o narrowing of intrevertebral foramen, disc compression 3.Dynamic angiogram: may show the compression 4. explores arterial complications (stenosis, aneurysms…)
- 30. 5. CT – MRA 3D technique 6. Dynamic phlebography
- 31. Electrophysiology Testing EMG & NCV • Electromyography& Nerve conduction study: may help to assess nervous ‘‘motor affection • somatosensory evoked responses
- 32. Arterial cervical outlet syndrome: compression of both subclavian and both vertebral arteries by scalenus anterior muscle magnetic resonance angiography
- 33. Computer reconstructed image of CT angiography 1- The right vertebral artery 2- The left hypoplastic vertebral artery 3- Site of compression of the left vertebral artery 4- Site of compression of the left subclavian artery 5- Site of compression of the right vertebral artery 6- Site of compression of the right subclavian artery
- 35. DD neurological sypmtoms • Carpel tunnel syndrome • Spinal canal tumors • Cervical spine strain sprain • Cervical disck disease • Cervical arthritis • Shoulder myositis • Angina pectoris • Raynaud's disease • Ulnar nerve compression – epicondylitis • Fibromyositis DD vascular symptoms • Other sources of emboli: Cardiac and aortic arch causes, coagulopathies • Vasculitis • Radiation-induced arteritis • Connective tissue disorders • Arterial dissection • Atherosclerotic disease • Traumatic
- 36. TREATMENT I. MEDICALTREATMENT • Analgesic treatment • Anti-inflammatory non steroid drugs • Muscle relaxing drugs • Weight reduction 2-PHYSICALTHERAPY Is the key of T.O.S. treatment Its purpose : 1- open the costo-clavicular space 2- fight against physiological shoulders falling attitude 3- Has to be progressive, painless, bilateral 4- Average duration : 3 to 6 months 5- If properly executed : 70 to 90% of good results
- 37. • Muscular relaxation • Neck stretches • Correct posture • Reinforce muscles that ‘‘open’’ the costo- clavicular space • Respiratory reduction • Avoid neck traction, weights, resistance exercises, strengthening exercises
- 39. ForNeurological symptoms • no improvement after several months • Live with symptoms • Surgical decompression ForVascular symptoms • Catheter-directed thrombolysis • Anticoagulation • Surgical decompression with intraoperative venography and subclavian vein PTA
- 40. 3-Surgerical decompression indicated: 1- When failure of physiotherapy 2- Neurologic compressions : sus-clavicular approach axillary approach 3- When osseous or musculo-ligamentar abnormalities: sub-clavicular approach 4-Non complicated arterial compressions: axillary approach 5- Complicated arterial compression (thrombosis, aneurysms…): sub-clavicular approach ± sub-clavicular approach 6- Complicated veinous compressions: difficult to choose
- 41. Complications Injury to • Subclavian artery/vein • Brachial plexus • Phrenic nerve • Long thoracic nerve • Thoracic duct • Sympathetic chain • Intercostal brachial cutaneous nerve (axillary) Pneumothorax Lymphleakage
- 42. Cervical rib resection & safe dividing
- 43. Adjuvantprocedures • Scalenectomy • Pectoralisminor tenotomy. • Sympathectomy
- 46. Recurrence
- 47. Tank Yu;)
- 48. ResearchTeam Datacollection & formating by: Yomna Ahmed Emad 561 Yasmin Magdy Metwally 559 Powerpoint by : Jasmin Magdy Mohammed 560 Presented by: Yasmin Essam Khalil 558 Group leader Dr Doaa Rifaat Supervised by Dr Fady Head department Dr Tarek Ezzat General Surgery Department, ZagazigUniversity Date :7 september ,2015