1) Combining ARBs and statins provides additive benefits for cardiovascular health by increasing NO levels, reducing oxidative stress and inflammation, lowering lipid levels, and decreasing endothelial dysfunction and insulin resistance through interacting mechanisms.
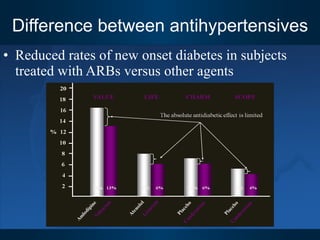
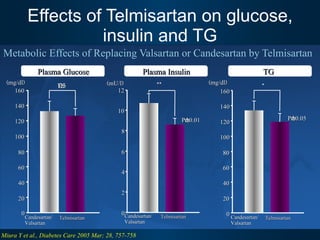
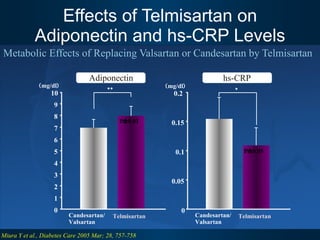
2) Telmisartan is particularly suitable for combination with statins as it has additional metabolic effects like improving glucose tolerance and reducing hs-CRP beyond other ARBs due to its PPAR-γ modulating properties.
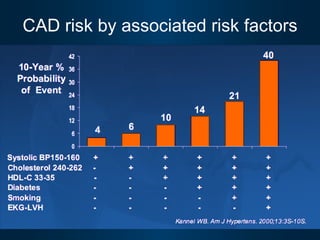
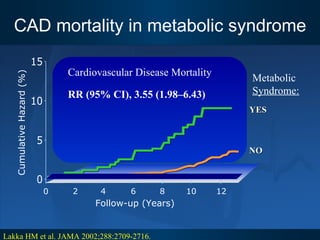
3) Patients who are hypertensive and have other cardiovascular risk factors like high cholesterol, diabetes, metabolic syndrome or a previous cardiovascular event are likely to benefit most from combination ARB/statin therapy.








![ARB+Statin after stenting Statins enhance the inhibitory effects of ARB on vascular neointimal formation in mice. The present case-control study investigated the efficacy of combined treatment with statin and ARB for preventing restenosis in patients with coronary artery disease. 210 patients with angina pectoris undergoing elective coronary stenting for de novo lesions of native coronary arteries were examined. All enrolled patients received aspirin and ticlopidine. The subjects were in 3 groups: no statin statin treatment without ARB Statin treatment with ARB. The rate of restenosis at 6 months after stent implantation in the statin group (19%) was significantly lower than that in the control group (32%). Study findings indicate that combined treatment with statin and ARB after stenting is a useful strategy for the prevention of coronary restenosis as patients treated with statins and ARBs were least likely [odds ratio (95% confidence interval): 0.30(0.12-0.74)] to develop coronary restenosis. Combined Treatment With Statin and ARB after Stenting for prevention of Coronary Restenosis, NISHIKAWA et al, J Cardiol, VOL.45;NO.3;PAGE.107-113(2005)](https://image.slidesharecdn.com/arbitelav-091126104613-phpapp01/85/ARB-Statin-28-320.jpg)