
Recommended
Recommended
More Related Content
Similar to BRIEF OBSERVATIONAll-cause Mortality Associated withTNF-a .docx
Similar to BRIEF OBSERVATIONAll-cause Mortality Associated withTNF-a .docx (20)
More from hartrobert670
More from hartrobert670 (20)
Recently uploaded
Recently uploaded (20)
BRIEF OBSERVATIONAll-cause Mortality Associated withTNF-a .docx
- 1. BRIEF OBSERVATION All-cause Mortality Associated with TNF-a Inhibitors in Rheumatoid Arthritis: A Meta-Analysis of Randomized Controlled Trials Lucile Poiroux, MD, Yannick Allanore, MD, PhD, André Kahan, MD, PhD, Jérôme Avouac, MD, PhD Paris Descartes University, Sorbonne Paris Cité, Rheumatology A Department, Cochin Hospital, Paris, France Funding: This Conflict of In Authorship: A conception, design Requests for re Université Paris D rue du Faubourg S E-mail address 0002-9343/$ -see http://dx.doi.org/1 ABSTRACT OBJECTIVE: To compare mortality data obtained from randomized controlled trials for the 5 tumor necrosis factor-a (TNF-a) inhibitors used in the treatment of rheumatoid arthritis. METHODS: A systematic review of articles published up to November 2014 was performed using electronic
- 2. databases. We included randomized, controlled trials, with a follow-up period of at least 24 weeks, comparing TNF-a inhibitors to placebo or disease-modifying antirheumatic drugs. The primary outcome was the occurrence of all-cause mortality. RESULTS: Twenty-three studies were selected. These articles included 6525 patients in the anti-TNF-a group and 3523 in the control group. The duration of patient follow-up ranged from 24 to 104 weeks. The risk of all-cause mortality in patients receiving TNF-a inhibitors was not significantly different from those receiving the comparator (odds ratio 1.32; 95% confidence interval, 0.76-2.29). Subgroup analyses with respect to the molecule used, the dose received, the use of TNF- a inhibitors as monotherapy or combination therapy, or the quality of the trial did not modify the findings. CONCLUSION: This meta-analysis performed on a large number of patients and including the 5 TNF-a inhibitors currently available shows no increased risk of medium-term all-cause mortality in patients with rheumatoid arthritis. � 2015 Elsevier Inc. All rights reserved. � The American Journal of Medicine (2015) -, --- KEYWORDS: Meta-analysis; Mortality; Rheumatoid arthritis; TNF-a inhibitors Tumor necrosis factor-a (TNF-a) inhibitors are the most widely used first-line biologic therapy for the treatment of rheumatoid arthritis. Much has been written on the concern that TNF-a inhibitors may increase the risk of malignancy, infections, and other serious adverse events.1,2 However, studies of the potential risks of this drug class on the “hard endpoint” mortality are scarce and have provided conflicting results.3 A previous meta-analysis reported no evidence of increased mortality associated with any TNF-a inhibitor in rheumatoid arthritis. However, the analysis was limited to research received no funding.
- 3. terest: None. ll authors had access to the data and participated in the , writing, editing, and final approval of the manuscript. prints should be addressed to Jérôme Avouac, MD, PhD, escartes, Service de Rhumatologie A, Hôpital Cochin, 27 aint-Jacques, Paris 75014, France. : [email protected] front matter � 2015 Elsevier Inc. All rights reserved. 0.1016/j.amjmed.2015.07.020 the 3 TNF-a inhibitors available at this period and mainly included short-term safety data.4 Thus, our aim was to assess the risk of medium-term all-cause mortality upon the 5 currently available TNF-a inhibitors in rheumatoid arthritis through a meta-analysis of randomized controlled trials. METHODS Data Sources and Literature Search We searched randomized controlled trials using MEDLINE via PubMed, the Cochrane databases, Embase, Google Scholar, and manual searches of reference lists from sys- tematic reviews and original publications. Studies published in English were identified from January 1, 2000 to November 1, 2014. The search terms included TNF alpha inhibitors; adalimumab; etanercept; certolizumab pegol; infliximab; golimumab; rheumatoid arthritis; Randomized controlled trials, mortality; English; All adults. Our mailto:[email protected] http://dx.doi.org/10.1016/j.amjmed.2015.07.020 2 The American Journal of Medicine, Vol -, No -, - 2015 research was limited to English language and human clinical trials.
- 4. Inclusion Criteria We defined the target population as adults with rheuma- CLINICAL SIGNIFICANCE � Tumor necrosis factor-a inhibitors show no increased risk of medium-term all- cause mortality. � The type of molecule and the dose received do not modify this finding. toid arthritis diagnosed according to the 1987 American College of Rheumatology criteria.5 In- terventions included all 5 currently available TNF-a inhibitors. Eligi- ble comparators included placebo and conventional disease-modifying antirheumatic drugs (DMARDs). The primary outcome of this study was the occurrence of all-cause mortality defined on an intention- to-treat basis. To better reflect the drug effect on the poten- tial risk of death, included studies have to report a minimum of 24 weeks of the study duration. Methodological Quality The articles that fulfilled the inclusion criteria underwent quality appraisal by using the Jadad scale.6 Data Extraction Two investigators (LP and JA) independently extracted data from articles using a customized form, available Figure 1 Flow diagram of articles evaluated for incl from the authors. Disagreements were resolved by consensus. Statistical Analysis
- 5. We used the Mantel-Haenszel method for calculating the usion and exclusion. RA ¼ r weighted summary odds ratio un- der the fixed-effect model. Next, the heterogeneity was incorpo- rated to calculate summary odds ratios under the random-effects model (DerSimonian and Laird).7 Statistical heterogeneity was tested by Q-test (c2) and I2 sta- tistic calculation.8 All statistical tests and creation of forest plots were conducted with MedCalc software (v11.4.4; Ostend, Belgium). Additional subgroup analyses were planned to check whether they would sub- stantially change the findings. RESULTS Included Studies The results of the article selection process are reported in Figure 1. Among the 495 studies initially analyzed, 23 studies fulfilled our inclusion criteria (Table 1).9-31 The median study duration was 46 weeks (range: 24 to 104 weeks). This analysis included 10,048 patients: 6525 were treated with TNF-a heumatoid arthritis. Table 1 Characteristics of Trials Included in the Analysis Reference Mean Disease Duration (Y) Placebo TNF-a Inhibitor
- 6. Trial Duration (Wk) Jadad Scoren Type Type Dose n Kremer et al, 20109 8.3 129 Methotrexate Golimumab 2-4 mg/kg/3 mo 257 48 4 Emery et al, 200910 3.4 160 Methotrexate Golimumab 50 or 100 mg/4 wk 318 24 5 Quinn et al, 200511 0.6 10 Methotrexate Infliximab 3 mg/kg 10 54 4 St. Clair et al, 200412 0.9 291 Methotrexate Infliximab 3 or 6 mg/kg 749 54 5 Keystone et al, 200413 11.0 200 Methotrexate Adalimumab 20 mg/wk or 40 mg/2 wk 419 52 3 Furst et al, 200314 10.4 318 Disease-modifying antirheumatic drugs Adalimumab 40 mg/2 wk 318 24 3 Smolen et al, 201315 6.8 200 Methotrexate Etanercept 25 or 50 mg/wk 404 28 5 Klareskog et al, 200416 6.8 228 Methotrexate Etanercept 25 mg/2 wk 231 52 4 Combe et al, 200617 6.2 50 Sulfasalazine Etanercept 25 mg/2 wk 101 24 3 Smolen et al, 200918 6.2 127 Methotrexate Certolizumab 200 mg or 400 mg/2 wk 492 24 3 Fleischmann et al, 200919 9.6 109 Placebo Certolizumab 400 mg/2 wk 111 24 5 Keystone et al, 200820 6.2 199 Methotrexate Certolizumab 200 or 400 mg/2 wk 783 52 4 Durez et al, 200721 0.4 14 Methotrexate Infliximab 3 mg/kg 15 46 2 Lipsky et al, 200022 10.6 88 Methotrexate Infliximab 3-10 mg/kg 340 52 3 Kavanaugh et al, 201323 0.3 517 Methotrexate Adalimumab 40 mg/2 wk 515 78 4
- 7. Van Vollenhoven et al, 201124 8.6 76 Methotrexate Adalimumab 40 mg/2 wk 79 26 2 Choy et al, 201225 9.6 121 Methotrexate Certolizumab 400 mg/2 wk 126 24 5 Breedveld et al, 200626 0.8 257 Methotrexate Adalimumab 40 mg/2 wk 268 52 3 Miyasaka et al, 200827 9.4 87 Placebo Adalimumab 20-40 mg or 80 mg/2 wk 265 24 3 van de Putte et al, 200428 10.9 110 Placebo Adalimumab 20-40 mg/wk or 2 wk 434 26 5 Schiff et al, 200829 7.7 110 Methotrexate Infliximab 3 mg/kg 165 24 4 Leirisalo-Repo et al, 201330 0.3 49 Disease-modifying antirheumatic drugs Infliximab 3 mg/kg 50 104 5 Bejarano et al, 200831 0.7 73 Methotrexate Adalimumab Not reported 75 56 5 TNF ¼ tumor necrosis factor. Poiroux et al TN F-a Inhibitors in Rheum atoid A
- 8. rthritis 3 Table 2 Events Reported in Trials Reference TNF-a Inhibitor Dose of TNF-a Inhibitor Deaths, n Cause of Death DosePlacebo TNF-a Inhibitor Placebo TNF-a Inhibitor Kremer et al, 20109 Golimumab 2-4 mg/kg/3 mos 0 1 0 Myocardial infarction Normal/high Emery et al, 200910 Golimumab 50 or 100 mg/4 wk 0 2 0 Suicide, cardiorespiratory arrest after surgery Normal/high Quinn et al, 200511 Infliximab 3 mg/kg 0 0 0 0 Normal St Clair et al, 200412 Infliximab 3 or 6 mg/kg 2 2 Respiratory failure due to methotrexate, upper gastrointestinal bleed Cardiac arrest, metastatic pancreatic cancer Normal/high
- 9. Keystone et al, 200413 Adalimumab 20 mg/wk or 40 mg/2 wk 0 3 0 Multiple fractures, urosepsis, complications of chemotherapy for lymphoma Normal Furst et al, 200314 Adalimumab 40 mg/2 wk 0 1 0 Necrotizing fasciitis Normal Smolen et al, 201315 Etanercept 25 or 50 mg/wk 0 2 0 Pulmonary embolism, septicemia Low/normal Klareskog et al, 200416 Etanercept 25 mg 2/wk 1 1 Pulmonary embolism Stroke and pneumonia Normal Combe et al, 200617 Etanercept 25 mg 2/wk 0 0 0 0 Normal Smolen et al, 200918 Certolizumab 200 mg or 400 mg/2 wk 0 2 0 Myocardial infarction, fracture and shock Low/normal Fleischmann et al, 200919 Certolizumab 400 mg/2 wk 0 0 0 0 Normal Keystone et al, 200820 Certolizumab 200 or 400 mg/2 wk 1 5 Myocardial infarction Hepatic neoplasm, cardiac arrest, cerebral stroke, myocardial necrosis, cardiac arrest Low/normal Durez et al, 200721 Infliximab 3 mg/kg 0 0 0 0 Normal Lipsky et al, 200022 Infliximab 3-10 mg/kg 3 5 Not reported Not reported Normal/high Kavanaugh et al, 201323 Adalimumab 40 mg/2 wk 1 6 Sudden death Septic shock, right ventricular
- 10. failure, unknown cause, acute respiratory distress, two interstitial lung disease Normal Van Vollenhoven et al, 201124 Adalimumab 40 mg/2 wk 0 0 0 0 Normal Choy et al, 201225 Certolizumab 400 mg/2 wk 0 0 0 0 Normal Breedveld et al, 200626 Adalimumab 40 mg/2 wk 1 1 Pneumonia Ovarian cancer Normal Miyasaka et al, 200827 Adalimumab 20-40 mg or 80 mg/2 wk 0 2 0 Interstitial lung disease, cerebral hemorrhage Low/normal/high van de Putte et al, 200428 Adalimumab 20-40 mg/wk or 2 wk 1 3 Complications of bowel obstruction Metastatic adenocarcinoma, cholangiocarcinoma, myocardial infarction Low/normal/high Schiff et al, 200829 Infliximab 3 mg/kg 0 1 0 Fibrosarcoma Normal Leirisalo-Repo et al, 201330 Infliximab 3 mg/kg 0 1 0 Not reported Normal Bejarano et al, 200831 Adalimumab Not reported 0 0 0 0 Not reported TNF ¼ tumor necrosis factor.
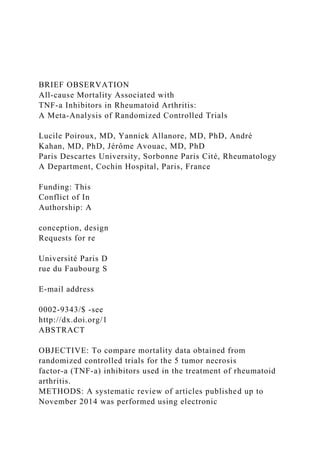
- 11. 4 The A m erican Journal of M edicine, Vol - , N o - , - 2015 Figure 2 Forest plot of trials comparing tumor necrosis factor-a inhibitors to comparators for the risk of all-cause mortality in patients with rheumatoid arthritis. Heterogeneity: Q ¼ 7.87; df ¼ 22, P ¼ .99, I2 < 25%. Poiroux et al TNF-a Inhibitors in Rheumatoid Arthritis 5 inhibitors and 3523 were treated with placebo or conventional DMARDs.
- 12. Primary Outcome: Mortality of Any Cause Upon TNF-a Inhibitors Compared with Controls During the study duration, 34/6525 (0.52%) deaths were observed in patients treated with TNF-a inhibitors, compared with 10/3523 (0.28%) deaths in those treated with conven- tional DMARDs/placebo (P ¼ .113) (Table 2).9-31 Thus, the risk of death of any cause in patients receiving TNF-a in- hibitors was not significantly different from those receiving the comparator (odds ratio [OR] 1.32; 95% confidence in- terval [CI], 0.76-2.29) (Figure 2). The results were consistent across trials (Q ¼ 7.87, P ¼ .99, and I2 < 25%). Subgroup analysis within the type of comparator did not modify previously observed results. The OR of mortality of patients receiving TNF-a inhibitors used as monotherapy vs placebo was 1.04 (95% CI, 0.20-5.34), and the OR of Table 3 Odds Ratio for All-cause Mortality According to the Molecule Total Adalimumab n ¼ 2373 Golimumab n ¼ 575 Rheumatoid arthritis (OR, 95% CI) 1.32 95% CI, 0.76-2.29 2.17 95% CI, 0.83-5.68
- 13. 2.02 95% CI, 0.23- CI ¼ confidence interval; OR ¼ odds ratio. mortality of patients receiving TNF-a inhibitors used in combination therapy vs conventional DMARDs was 1.36 (95% CI, 0.76-2.43). Secondary Analyses Subgroup Analyses with Respect to Each Molecule. Individually, each molecule analyzed separately did not show an increased risk of mortality of any cause (Table 3). Subgroup Analysis with Respect to the Dose of TNF-a Inhibitors. To address the potential dose impact, we com- pared the mortality event rates according to TNF-a inhibitor dose (high dose, defined by a dose higher than usual TNF-a inhibitor dose as per package insert, vs usual dose). High dose of TNF-a inhibitors was not significantly associated with a significant increase in risk of mortality (OR 0.97; 95% CI, 0.26-3.54 vs 1.43; 95% CI, 0.79-2.59 for the usual dose). Used Certolizumab n ¼ 1512 Infliximab n ¼ 1329 Etanercept n ¼ 736 18.19 1.19 95% CI, 0.27-5.18
- 14. 0.70 95% CI, 0.27-1.81 1.28 95% CI, 0.23-7.25 6 The American Journal of Medicine, Vol -, No -, - 2015 Subgroup Analysis with Respect to the Quality of Evi- dence. Most of our comparison analyses reached a high level of quality of evidence, with a mean Jadad score of 3.87 � 1.01 (Table 1).9-31 We compared studies with a high quality (Jadad score >3) to those with a lower quality (Jadad score �3). The results did not appear to differ substantially. In high-quality studies, the OR for mortality of any cause was 1.60 (95% CI, 0.78-3.30), and in lower-quality studies, the OR was 0.99 (95% CI, 0.42-2.31). To help address the potential impact of the calendar time, we also compared mortality according to calendar year of publication (before and after 2006). The summary ORs for mortality were both not significant for these 2 time pe- riods (0.80; 95% CI, 0.37-1.76 before and 2.03; 95% CI, 0.91-4.52 after 2006). DISCUSSION A recent meta-analysis has underlined the higher risk of overall serious adverse events in certolizumab pegol-treated patients and the significant increase in the risk of serious infections in patients on adalimumab, certolizumab pegol, and infliximab, which might suggest a potential higher risk of mortality.1 This hypothesis has not been confirmed in our meta-analysis, which covered the same time period and compared the 5 currently available TNF-a inhibitors for the risk of mortality, an undisputed hard endpoint. Indeed, the
- 15. use of TNF-a inhibitors is not associated in our study with an increased risk of medium-term mortality. Several registries have suggested a reduction of the risk of mortality in patients with rheumatoid arthritis treated with TNF-a inhibitors.32-34 Several factors may explain this discrepancy, especially the inclusion of highly selected patients in randomized controlled trials compared with unse- lected patients in registries, and the longer time of drug exposure in the latter. This may suggest that registries may be more adequate to address the impact of TNF-a inhibitors on overall mortality. However, our results are consistent with data extractedfromtheBritishSocietyforRheumatologyBiologics Registers and with the meta-analysis of Leombruno.4,35 Strengths of our meta-analysis are its large sample size, an indirect comparison among the 5 available molecules, the presence of a control group obtained through a process of randomization, the quality of data extracted from a majority of high-quality randomized controlled trials, and the absence of heterogeneity among included trials. Limitations of our meta- analysis included the generalization of our results and the absence of long-term exposition on TNF-a inhibitors. Insuf- ficient data were provided to perform a subgroup analysis according to the duration of use of TNF-a inhibitors. More- over, effect of TNF-a inhibitors on mortality may occur after discontinuation of these drugs, and this aspect could not be assessed in our meta-analysis. In conclusion, this meta-analysis shows that treatment with TNF-a inhibitors is not associated with a higher risk of medium-term mortality of any cause in patients with rheumatoid arthritis. These results are reassuring for this duration, given that these therapies are highly effective at controlling symptoms and reducing disability and damage. Further studies are warranted to assess the long-term effect
- 16. of TNF-a inhibitors on mortality. References 1. Michaud TL, Rho YH, Shamliyan T, Kuntz KM, Choi HK. The comparative safety of TNF inhibitors in rheumatoid arthritis: a meta- analysis update of 44 randomized controlled trials. Am J Med. 2014;127(12):1208-1232. 2. Haynes K, Beukelman T, Curtis JR, et al. Tumor necrosis factor a inhibitor therapy and cancer risk in chronic immune-mediated diseases. Arthritis Rheum. 2013;65(1):48-58. 3. Herrinton LJ, Liu L, Chen L, et al. Association between anti- TNF-a therapy and all-cause mortality. Pharmacoepidemiol Drug Saf. 2012;21(12):1311-1320. 4. Leombruno JP, Einarson TR, Keystone EC. The safety of anti-tumour necrosis factor treatments in rheumatoid arthritis: meta and exposure- adjusted pooled analyses of serious adverse events. Ann Rheum Dis. 2009;68(7):1136-1145. 5. Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315-324. 6. Avouac J, Vicaut E, Bardin T, et al. Efficacy of joint lavage
- 17. in knee osteoarthritis: meta-analysis of randomized controlled studies. Rheu- matology (Oxford). 2010;49(2):334-340. 7. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177-178. 8. Higgins JPT, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-560. 9. Kremer J, Ritchlin C, Mendelsohn A, et al. Golimumab, a new human anti-tumor necrosis factor a antibody, administered intravenously in patients with active rheumatoid arthritis: forty-eight-week efficacy and safety results of a phase III randomized, double-blind, placebo- controlled study. Arthritis Rheum. 2010;62(4):917-928. 10. Emery P, Fleischmann RM, Moreland LW, et al. Golimumab, a human anti-tumor necrosis factor a monoclonal antibody, injected subcuta- neously every four weeks in methotrexate-naive patients with active rheumatoid arthritis: twenty-four-week results of a phase III, multi- center, randomized, double-blind, placebo-controlled study of goli- mumab before methotrexate as first-line therapy for early-onset rheumatoid arthritis. Arthritis Rheum. 2009;60(8):2272-2283. 11. Quinn MA, Conaghan PG, O’Connor PJ, et al. Very early
- 18. treatment with infliximab in addition to methotrexate in early, poor- prognosis rheumatoid arthritis reduces magnetic resonance imaging evidence of synovitis and damage, with sustained benefit after infliximab with- drawal: results from a twelve-month randomized, double-blind, pla- cebo-controlled trial. Arthritis Rheum. 2005;52(1):27-35. 12. St. Clair EW, van der Heijde DMFM, Smolen JS, et al. Combination of infliximab and methotrexate therapy for early rheumatoid arthritis: a randomized, controlled trial. Arthritis Rheum. 2004;50(11):3432-3443. 13. Keystone EC, Kavanaugh AF, Sharp JT, et al. Radiographic, clinical, and functional outcomes of treatment with adalimumab (a human anti- tumor necrosis factor monoclonal antibody) in patients with active rheumatoid arthritis receiving concomitant methotrexate therapy: a randomized, placebo-controlled, 52-week trial. Arthritis Rheum. 2004;50(5):1400-1411. 14. Furst DE, Schiff MH, Fleischmann RM, et al. Adalimumab, a fully human anti tumor necrosis factor-alpha monoclonal antibody, and concomitant standard antirheumatic therapy for the treatment of rheu- matoid arthritis: results of STAR (Safety Trial of Adalimumab
- 19. in Rheumatoid Arthritis). J Rheumatol. 2003;30(12):2563-2571. 15. Smolen JS, Nash P, Durez P, et al. Maintenance, reduction, or with- drawal of etanercept after treatment with etanercept and methotrexate in patients with moderate rheumatoid arthritis (PRESERVE): a rand- omised controlled trial. Lancet. 2013;381(9870):918-929. http://refhub.elsevier.com/S0002-9343(15)00697-X/sref1 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref1 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref1 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref1 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref2 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref2 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref2 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref3 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref3 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref3 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref4 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref4 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref4 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref4 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref5 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref5 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref5 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref6 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref6 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref6 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref7 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref7 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref8 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref8 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref9
- 21. APPENDIX Supplementary references accompanying this article can be found in the online version at http://dx.doi.org/10.1016/ j.amjmed.2015.07.020. Poiroux et al TNF-a Inhibitors in Rheumatoid Arthritis 7 16. Klareskog L, van der Heijde D, de Jager JP, et al. Therapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double- blind randomised controlled trial. Lancet. 2004;363(9410):675-681. 17. Combe B. Etanercept and sulfasalazine, alone and combined, in pa- tients with active rheumatoid arthritis despite receiving sulfasalazine: a double-blind comparison. Ann Rheum Dis. 2006;65(10):1357- 1362. 18. Smolen J, Landewé RB, Mease P, et al. Efficacy and safety of certo- lizumab pegol plus methotrexate in active rheumatoid arthritis: the RAPID 2 study. A randomised controlled trial. Ann Rheum Dis. 2009;68(6):797-804. 19. Fleischmann R, Vencovsky J, van Vollenhoven RF, et al. Efficacy and safety of certolizumab pegol monotherapy every 4 weeks in patients with rheumatoid arthritis failing previous disease-modifying antirheu- matic therapy: the FAST4WARD study. Ann Rheum Dis.
- 22. 2009;68(6): 805-811. 20. Keystone E, Heijde DVD, Mason D, et al. Certolizumab pegol plus methotrexate is significantly more effective than placebo plus metho- trexate in active rheumatoid arthritis: findings of a fifty-two- week, phase III, multicenter, randomized, double-blind, placebo- controlled, parallel-group study. Arthritis Rheum. 2008;58(11):3319-3329. 21. Durez P, Malghem J, Toukap AN, et al. Treatment of early rheumatoid arthritis: a randomized magnetic resonance imaging study comparing the effects of methotrexate alone, methotrexate in combination with infliximab, and methotrexate in combination with intravenous pulse methylprednisolone. Arthritis Rheum. 2007;56(12):3919-3927. 22. Lipsky PE, van der Heijde DM, St. Clair EW, et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. N Engl J Med. 2000;343(22):1594-1602. 23. Kavanaugh A, Fleischmann RM, Emery P, et al. Clinical, functional and radiographic consequences of achieving stable low disease activity and remission with adalimumab plus methotrexate or methotrexate alone in early rheumatoid arthritis: 26-week results from the
- 23. rando- mised, controlled OPTIMA study. Ann Rheum Dis. 2013;72(1):64-71. 24. Van Vollenhoven RF, Kinnman N, Vincent E, Wax S, Bathon J. Atacicept in patients with rheumatoid arthritis and an inadequate response to methotrexate: results of a phase II, randomized, placebo- controlled trial. Arthritis Rheum. 2011;63(7):1782-1792. 25. Choy E, McKenna F, Vencovsky J, et al. Certolizumab pegol plus MTX administered every 4 weeks is effective in patients with RA who are partial responders to MTX. Rheumatology. 2012;51(7):1226-1234. 26. Breedveld FC, Weisman MH, Kavanaugh AF, et al. The PREMIER study: a multicenter, randomized, double-blind clinical trial of com- bination therapy with adalimumab plus methotrexate versus metho- trexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum. 2006;54(1):26-37. 27. Miyasaka N. The CHANGE Study Investigators. Clinical investigation in highly disease-affected rheumatoid arthritis patients in Japan with adalimumab applying standard and general evaluation: the
- 24. CHANGE study. Mod Rheumatol. 2008;18(3):252-262. 28. van de Putte LB, Atkins C, Malaise M, et al. Efficacy and safety of adalimumab as monotherapy in patients with rheumatoid arthritis for whom previous disease modifying antirheumatic drug treatment has failed. Ann Rheum Dis. 2004;63(5):508-516. 29. Schiff M, Keiserman M, Codding C, et al. Efficacy and safety of abatacept or infliximab vs placebo in ATTEST: a phase III, multi- centre, randomised, double-blind, placebo-controlled study in patients with rheumatoid arthritis and an inadequate response to methotrexate. Ann Rheum Dis. 2008;67(8):1096-1103. 30. Leirisalo-Repo M, Kautiainen H, Laasonen L, et al. Infliximab for 6 months added on combination therapy in early rheumatoid arthritis: 2- year results from an investigator-initiated, randomised, double- blind, placebo-controlled study (the NEO-RACo Study). Ann Rheum Dis. 2013;72(6):851-857. 31. Bejarano V, Quinn M, Conaghan PG, et al. Effect of the early use of the anti-tumor necrosis factor adalimumab on the prevention of job loss in patients with early rheumatoid arthritis. Arthritis Rheum.
- 25. 2008;59(10):1467-1474. 32. Jacobsson LT, Turesson C, Nilsson JA, et al. Treatment with TNF blockers and mortality risk in patients with rheumatoid arthritis. Ann Rheum Dis. 2007;66(5):670-675. 33. Carmona L, Descalzo MA, Perez-Pampin E, et al. All-cause and cause- specific mortality in rheumatoid arthritis are not greater than expected when treated with tumour necrosis factor antagonists. Ann Rheum Dis. 2007;66(7):880-885. 34. Listing J, Kekow J, Manger B, et al. Mortality in rheumatoid arthritis: the impact of disease activity, treatment with glucocorticoids, TNFa inhibitors and rituximab. Ann Rheum Dis. 2015;74(2):415-421. 35. Lunt M, Watson KD, Dixon WG, et al. No evidence of association between anti-tumor necrosis factor treatment and mortality in patients with rheumatoid arthritis: results from the British Society for Rheumatology Biologics Register. Arthritis Rheum. 2010;62: 3145-3153. http://refhub.elsevier.com/S0002-9343(15)00697-X/sref16 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref16 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref16 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref16 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref17 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref17
- 28. http://refhub.elsevier.com/S0002-9343(15)00697-X/sref34 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref35 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref35 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref35 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref35 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref35 http://dx.doi.org/10.1016/j.amjmed.2015.07.020 http://dx.doi.org/10.1016/j.amjmed.2015.07.020 Appendix 1: References of included studies 1. Kremer J, Ritchlin C, Mendelsohn A, Baker D, Kim L, Xu Z, et al. Goli- mumab, a new human anti-tumor necrosis factor a antibody, administered intravenously in patients with active rheumatoid arthritis: Forty-eight- week efficacy and safety results of a phase III randomized, double-blind, placebo-controlled study. Arthritis Rheum. 2010;62(4):917-928. 2. Emery P, Fleischmann RM, Moreland LW, Hsia EC, Strusberg I, Durez P, et al. Golimumab, a human anti-tumor necrosis factor a monoclonal antibody, injected subcutaneously every four weeks in methotrexate-naive patients with active rheumatoid arthritis: Twenty- four-week results of a phase III, multicenter, randomized, double- blind, placebo-controlled study of golimumab before methotrexate as first-line therapy for early-onset rheumatoid arthritis. Arthritis Rheum. 2009;60(8):2272-2283.
- 29. 3. Quinn MA, Conaghan PG, O’Connor PJ, Karim Z, Greenstein A, Brown A, et al. Very early treatment with infliximab in addition to methotrexate in early, poor-prognosis rheumatoid arthritis reduces magnetic resonance imaging evidence of synovitis and damage, with sustained benefit after infliximab withdrawal: Results from a twelve- month randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2005;52(1):27-35. 4. St. Clair EW, van der Heijde DMFM, Smolen JS, Maini RN, Bathon JM, Emery P, et al. Combination of infliximab and metho- trexate therapy for early rheumatoid arthritis: A randomized, controlled trial. Arthritis Rheum. 2004;50(11):3432-3443. 5. Keystone EC, Kavanaugh AF, Sharp JT, Tannenbaum H, Hua Y, Teoh LS, et al. Radiographic, clinical, and functional outcomes of treatment with adalimumab (a human anti-tumor necrosis factor monoclonal antibody) in patients with active rheumatoid arthritis receiving concomitant methotrexate therapy: A randomized, placebo- controlled, 52-week trial. Arthritis Rheum. 2004;50(5):1400- 1411. 6. Furst DE, Schiff MH, Fleischmann RM, Strand V, Birbara CA,
- 30. Compagnone D, et al. Adalimumab, a fully human anti tumor necrosis factor-alpha monoclonal antibody, and concomitant standard anti- rheumatic therapy for the treatment of rheumatoid arthritis: results of STAR (Safety Trial of Adalimumab in Rheumatoid Arthritis). J Rheumatol. 2003;30(12):2563-2571. 7. Smolen JS, Nash P, Durez P, Hall S, Ilivanova E, Irazoque- Palazuelos F, et al. Maintenance, reduction, or withdrawal of etanercept after treatment with etanercept and methotrexate in patients with moderate rheumatoid arthritis (PRESERVE): a randomised controlled trial. The Lancet. 2013;381(9870):918-929. 8. Klareskog L, van der Heijde D, de Jager JP, Gough A, Kalden J, Malaise M, et al. Therapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double-blind randomised controlled trial. Lancet. 2004;363(9410):675-681. 9. Combe B. Etanercept and sulfasalazine, alone and combined, in pa- tients with active rheumatoid arthritis despite receiving sulfasalazine: a double-blind comparison. Ann Rheum Dis. 2006;65(10):1357- 1362.
- 31. 10. Smolen J, Landewé RB, Mease P, Brzezicki J, Mason D, Luijtens K, et al. Efficacy and safety of certolizumab pegol plus methotrexate in active rheumatoid arthritis: the RAPID 2 study. A randomised controlled trial. Ann Rheum Dis. 2009;68(6):797-804. 11. Fleischmann R, Vencovsky J, van Vollenhoven RF, Borenstein D, Box J, Coteur G, et al. Efficacy and safety of certolizumab pegol monotherapy every 4 weeks in patients with rheumatoid arthritis failing previous disease-modifying antirheumatic therapy: the FAST4WARD study. Ann Rheum Dis. 2009;68(6):805-811. 12. Keystone E, Heijde DVD, Mason D, Landewé R, Vollenhoven RV, Combe B, et al. Certolizumab pegol plus methotrexate is significantly more effective than placebo plus methotrexate in active rheumatoid arthritis: Findings of a fifty-two-week, phase III, multicenter, ran- domized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum. 2008;58(11):3319-3329. 13. Durez P, Malghem J, Toukap AN, Depresseux G, Lauwerys BR, Westhovens R, et al. Treatment of early rheumatoid arthritis: A ran- domized magnetic resonance imaging study comparing the effects of methotrexate alone, methotrexate in combination with
- 32. infliximab, and methotrexate in combination with intravenous pulse methylpredniso- lone. Arthritis Rheum. 2007;56(12):3919-3927. 14. Lipsky PE, van der Heijde DM, St. Clair EW, Furst DE, Breedveld FC, Kalden JR, et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. N Engl J Med. 2000;343(22):1594-1602. 15. Kavanaugh A, Fleischmann RM, Emery P, Kupper H, Redden L, Guerette B, et al. Clinical, functional and radiographic consequences of achieving stable low disease activity and remission with adalimumab plus methotrexate or methotrexate alone in early rheumatoid arthritis: 26-week results from the randomised, controlled OPTIMA study. Ann Rheum Dis. 2013;72(1):64-71. 16. Van Vollenhoven RF, Kinnman N, Vincent E, Wax S, Bathon J. Atacicept in patients with rheumatoid arthritis and an inadequate response to methotrexate: Results of a phase II, randomized, placebo- controlled trial. Arthritis Rheum. 2011;63(7):1782-1792. 17. Choy E, McKenna F, Vencovsky J, Valente R, Goel N, VanLunen B, et al. Certolizumab pegol plus MTX administered every 4 weeks is effective in patients with RA who are partial responders to
- 33. MTX. Rheumatology. 2012;51(7):1226-1234. 18. Breedveld FC, Weisman MH, Kavanaugh AF, Cohen SB, Pavelka K, Vollenhoven Rv, et al. The PREMIER study: A multicenter, ran- domized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adali- mumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum. 2006;54(1):26-37. 19. Miyasaka N. The CHANGE Study Investigators. Clinical investigation in highly disease-affected rheumatoid arthritis patients in Japan with adalimumab applying standard and general evaluation: the CHANGE study. Mod Rheumatol. 2008;18(3):252-262. 20. Van de Putte LBA. Efficacy and safety of adalimumab as monotherapy in patients with rheumatoid arthritis for whom previous disease modifying antirheumatic drug treatment has failed. Ann Rheum Dis. 2004;63(5):508-516. 21. Schiff M, Keiserman M, Codding C, Songcharoen S, Berman A, Nayiager S, et al. Efficacy and safety of abatacept or infliximab vs placebo in ATTEST: a phase III, multi-centre, randomised, double-
- 34. blind, placebo-controlled study in patients with rheumatoid arthritis and an inadequate response to methotrexate. Ann Rheum Dis. 2008;67(8):1096-1103. 22. Leirisalo-Repo M, Kautiainen H, Laasonen L, Korpela M, Kauppi MJ, Kaipiainen-Seppänen O, et al. Infliximab for 6 months added on combination therapy in early rheumatoid arthritis: 2- year results from an investigator-initiated, randomised, double-blind, placebo- controlled study (the NEO-RACo Study). Ann Rheum Dis. 2013;72(6):851- 857. 23. Bejarano V, Quinn M, Conaghan PG, Reece R, Keenan A-M, Walker D, et al. Effect of the early use of the anti-tumor necrosis factor adalimumab on the prevention of job loss in patients with early rheu- matoid arthritis. Arthritis Rheum. 2008;59(10):1467-1474. 7.e1 The American Journal of Medicine, Vol -, No -, - 2015 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref36 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref36 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref36 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref36 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref36 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref37 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref37 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref37 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref37 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref37 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref37 http://refhub.elsevier.com/S0002-9343(15)00697-X/sref37
- 38. SearchInclusion CriteriaMethodological QualityData ExtractionStatistical AnalysisResultsIncluded StudiesPrimary Outcome: Mortality of Any Cause Upon TNF-α Inhibitors Compared with ControlsSecondary AnalysesSubgroup Analyses with Respect to Each MoleculeSubgroup Analysis with Respect to the Dose of TNF-α InhibitorsSubgroup Analysis with Respect to the Quality of EvidenceDiscussionReferencesAppendixAppendix 1: References of included studies Neurourology and Urodynamics 24:267^272 (2005) Acupuncture for Nocturnal Enuresis in Children: A Systematic Review and Exploration of Rationale Wendy F. Bower,1* M. Diao,1 J.L. Tang,2,3 and C.K. Yeung1 1Department of Surgery, Division of Paediatric Surgery and Paediatric Urology, The Chinese University of Hong Kong, Hong Kong 2Department of Community and Family Medicine, The Chinese University of Hong Kong, Hong Kong 3Hong Kong Branch of the Chinese Cochrane Centre, The Chinese University of Hong Kong, Hong Kong Objectives: This review identi¢ed reports of acupuncture for childhood nocturnal enuresis, with the aim of ascertaining whether acupuncture is e⁄cacious and or better than standard therapy for treating enuresis. Materials and Methods: Studies of children of either gender <18 years of age who received acupuncture treatment for nocturnal enuresis, were considered. The primary outcome
- 39. measure was change in the mean number of wet episodes following treatment. Electronic searching was supplemented by hand searching of western medicine and traditional Chinese medicine (TCM) journals along with English language alternative medicine journals. Trials were assessed for quality and sources of bias. Meta-analysis was performed and the overall weighted odds ratio (OR) and associated 95% con¢dence interval (CI) were computed using the ¢xed e¡ect model; the Forest plot was used to demonstrate results. Results: Two hundred six abstracts were identi¢ed, of which 11 studies were eligible for data extraction. All the trials were of low methodological quality.There was some evidence that acupuncture is useful for nocturnal enuresis when used in conjunction with other treatment that may also include a di¡erent form of acupuncture (OR 3.98, CI: 2.2^7.2). When one form of acupuncture is compared with another there was marked heterogeneity, implying that some forms of acupuncture are e¡ective. Conclusion: This review provides tentative evidence for the e⁄cacy of acupuncture for the treatment of childhood nocturnal enuresis. Due to the low meth- odological quality of studies, evidence to identify, which parameters of acupuncture work best, is lacking. More rigorous trials are clearly warranted. Neurourol. Urodynam. 24:267 ^272, 2005. � 2005 Wiley-Liss, Inc. Key words: acupuncture;Chinesemedicine;meta- analysis;nocturnalenuresis INTRODUCTION Current treatment of nocturnal enuresis includes chemical
- 40. manipulation of neuromuscular structures and diuresis, and behavioral initiatives to impact arousal and bladder storage. Traditional Chinese medicine (TCM) claims that Chinese acupuncture induces a decrease in the number of wet epi- sodes (by 76% and 98% [Zhong, 1986; Tuzuner et al., 1989]), improves bladder storage capacity, and enhances arousal from sleep in order to void [Bjorkstrom et al., 2000; Serel et al., 2001; Honjo et al., 2002]. A reduction in uninhibited bladder contractions has also been reported following acu- puncture [Minni et al., 1990; Kachan et al., 1993]. Acupuncture is believed to normalize bladder function by invigorating the kidney, spleen and brain, calming the mind, and adjusting Qi of the lungs, vital energy and blood. The word itself is originally derived from Latin and refers to ‘‘piercing with a sharp instrument.’’ The practice utilizes the concept of 12 primary meridians or energy channels along which are distributed 360 acupuncture points. Each point is located in an area of low electrical resistance and sites used to treat bladder dysfunction appear to coincide with innerva- tion by spinal sacral segments S2 through S4. Stimulation of these acupoints by manual pressure, penetration of the skin, heating, the application of laser, electrotherapy, or moxibus- tion is thought to induce homeostatic changes [Berman, 2001]. Most practitioners agree that optimal results will be obtained if a patient experiences the spread of treatment sen- sation (including numbness, heaviness, distension, and sore- ness) beyond the acupuncture site, a condition known as deqi [Wu et al., 1999; Hui et al., 2000]. This review aimed to identify reports across both Asian and English language literature relating to the use of acu- puncture for nocturnal enuresis in children and to perform meta-analyses.The speci¢c objectives were to ascertain if acu- puncture is e⁄cacious and or better than standard therapy
- 41. *Correspondence to: Wendy F. Bower, Department of Surgery, Division of Paediatric Surgery and Paediatric Urology,The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, NT, Hong Kong. E-mail: [email protected] Received 27 July 2004; Accepted 2 December 2004 Published online 24 March 2005 inWiley InterScience (www.interscience.wiley.com) DOI 10.1002/nau.20108 � 2005 Wiley-Liss, Inc. for enuresis, and also to identify and explore any sources of heterogeneity. MATERIALS AND METHODS Studies of children of either gender, who were under the age of 18 years and received acupuncture treatment for noc- turnal enuresis, were considered. Studies were excluded if they considered adults, neurogenic bladder dysfunction, patients with active infection/in£ammation/implanted neu- romodulating devices or structural/metabolic disorders ren- dering function of the urinary tract atypical. Electrotherapy intervention applied away from recognized bladder/spleen/ kidney acupuncture points was also an exclusion criteria. As it is di⁄cult to include a sham or placebo group in acupuncture studies only a small number of randomized controlled trials were expected, and the review therefore included non-randomized trials of acupuncture, prospective cohorts, and alternative allocation trials.
- 42. ‘‘Acupuncture’’ treatment required needles to be inserted into acupoints; twisting, pressure application, moxibustion (the application of heat resulting from the burning of a small bundle of tightly bound herbs over targeted acupoints), or additional electrical current was also accepted. The review initially sought to di¡erentiate between techniques, combina- tion of points used, and treatment frequency and duration. The primary outcome measure was change in number of wet nights per week following cessation of acupunc- ture. Studies reported this as cure, however the de¢nition was not uniformly stated. A secondary measure planned was change in number of spontaneous arousals to void per week. Adverse events were also considered. The search covered the period 1980^2003 and considered trials reported in any language, with a focus on studies described in Chinese and other Asian languages. The follow- ing data sources were searched electronically: Cochrane Controlled Trials Register; Complimentary medicine ¢eld of Cochrane collaboration; MEDLINE (1980^2003); EMBASE (1980^2003); CISCOM; NCCAM; PROQUEST; DARE; AMED; ACME; CMB: Chinese Biomedical Disk; Japanese medical database. Hand searching was undertaken in 23 Wes- tern Medicine Chinese Journals, 11 TCM Journals and 6 English language alternative medicine journals, and regional and national acupuncture conference proceedings. Review papers were scrutinized, along with reference lists from iden- ti¢ed trials. Keywords used in the electronic search included: acu- puncture; complimentary medicine; alternative medicine; fringe medicine; acupressure; acustimulation; needle acu- puncture; needling; moxibustion; TCM; Chinese medicine; incontinence; bladder dysfunction; voiding dysfunction;
- 43. enuresis; nocturnal enuresis; overactive bladder; detrusor instability; urge incontinence; urge syndrome. The search strategy speci¢ed randomized controlled trials/random allo- cation/clinical trials/placebo or sham trials. Two investigators scrutinized abstracts, obtained hard copies to assess eligibility, and coded relevant trials before data extraction. Study details were examined separately and classi¢ed on the basis of methodology. Study eligibility de- tails noted included: type of study, participants, intervention, control and outcome measures. Data was extracted using a standardized form. Trials were scrutinized for quality aspects known to be associated with sources of bias: allocation concealment, ran- domization, blinding of assessors, subjects and data analysis personnel, intention-to-treat analysis and withdrawal or loss to follow-up. The Jadad score was used to the measure reduc- tion of bias [Jadad et al., 1996]. Maximum possible score on this instrument is 5 and the minimum, indicating the highest level of bias, is zero. Heterogeneity was explored using subgroup analysis [DerSimonian and Laird, 1986]. The methodological quality was identi¢ed as one of the determinants of heterogeneity and assessed similarly. Given the large heterogeneity the overall weighted odds ratio (OR) and the associated 95% con- ¢dence interval (CI) were computed by using the random e¡ect model. The Forest plot was used to demonstrate the details of the results. Statistical analysis utilized SAS. RESULTS Electronic searching of the Chinese databases revealed 129 potentially eligible abstracts describing the use of acu- puncture for nocturnal enuresis. English electronic databases
- 44. revealed 50 abstracts, of which 17 were considered possible trials and retrieved for scrutiny. After hand-searching a further 27 potentially eligible abstracts were identi¢ed. In total 206 abstracts were available. After rejecting papers that did not actually consider children, did not describe results, used concomitant co-interventions, reported only day symp- toms, or included less than 10 subjects, 84 potentially eligible studies remained. Of these, 75 studies originated from main- land China, 2 from Japan and 7 from Europe. Table I describes the characteristics of the 84 studies iden- ti¢ed. It can be seen that only 11 studies were ultimately eli- gible for review and analysis, whilst the rest were excluded because of single group design, lack of relevance to nocturnal enuresis, comparison of di¡erent forms of acupuncture, and lack of outcome measures. Table II summarizes the key char- acteristics of the eligible studies: type of comparison, dura- tion of treatment, length of follow-up, and rate of cure. None of the studies attempted to sub-classify enuresis. No authors reported baseline or post-treatment measures of arousal to void at night, and there was a similar lack of reported adverse events. A secondary aim of the review was to identify and explore sources of heterogeneity. However, study design was uniformly poor and both description of symptoms and mode of application of acupuncture were inadequate, preventing further analysis. 268 Bower et al. Table III shows the quality of each trial as scored accord- ing to the Jadad criteria. As the maximum individual study score is 5, it can be seen that all the trails failed to meet evi- dence-based medicine levels of bias minimization. None of
- 45. the studies reported the use of placebo or sham acupuncture. Whilst patients were allocated to di¡erent treatment groups, randomization methods were not discussed by any of the authors. Figure 1 shows the meta-analysis forest plot for enuresis cure in three studies (four comparisons, only one study ran- domized) that considered acupuncture in conjunction with another therapy when compared to the other therapy alone. The combined results show that acupuncture can further sig- ni¢cantly reduce the number of wet nights when used in addition to either another form of acupuncture or Chinese herbal medicine. The Funnel plot and symmetrical testing showed no obvious evidence of publication bias. The comparison of conventional acupuncture and another acupuncture or Chinese therapy is reported in Figure 2. Whilst there was no overall signi¢cant di¡erence, (which is well expected given the nature of comparisons), there is obvious heterogeneity among the studies suggesting that some forms of acupuncture might be more e¡ective than others. An examination of the individual studies showed: (1) conventional acupuncture was signi¢cantly better than both normal saline injections over acupoints (B2) and auri- cular seed embedding (B3); neither of these two studies being randomized. (2) Acupuncture was signi¢cantly less e¡ective than needle embedding (B8) and vitamin injections (B9); both of these studies being randomized. The asymme- try test of the funnel plot did not suggest obvious publication bias. The ¢nal meta-analysis compared laser acupuncture with the current gold-standard medication used in the manage- ment of nocturnal enuresis. It can be seen from Figure 3 that the outcome favors medication but was not signi¢cantly
- 46. better than acupuncture. TABLE I. Characteristics of Papers Considered for Eligibility of Inclusion in Systematic Review Study characteristics Number of studies excluded Number of studies included Single group design 56 Comparison between two di¡erent forms of acupuncture 6 Not a trial 2 Not relating to enuresis 9 Acupuncture as the control group 3 Acupuncture compared to another traditional Chinese medicine (TCM) treatment 7 Acupuncture compared to western medication 1 Total 73 11 TABLE II. Subjects, Comparison Intervention, and Results Reported in Trials of Acupuncture for Nocturnal Enuresis Author(s) and year
- 47. of publication Number of subjects Type of comparison Duration of treatment (** not stated) Follow-up post treatment Cure with acupuncture (%) Cure with comparative treatment (%) Cai [1987] 361 Acupuncture versus auricular needle embedding (B1) ** 1 month 97/193 (50) 41/108 (38) Acupuncture versus saline injection (B2) 97/193 (50) 14/60 (23) Ji and Zhou [2000] 138 Acupuncture and auricular seed embedding versus auricular seed embedding (A1) ** 6 months 29/37 (78) 17/49 (35) Acupuncture versus auricular seed embedding (B3) 35/52 (67) 17/49 (35) Li and Xue [1996] 96 Acupuncture versus catgut embedding (B4) ** 6 months 13/32 (41) 35/64 (55) Liu and Shen [1990] 110 Acupuncture versus photomagnetic
- 48. laser (B5) 2 weeks 6 months 38/52 (73) 44/58 (76) Lu [2000] 97 Head and body acupuncture and auricular seed embedding versus body acupuncture and auricular seed embedding (A2) 4 weeks 6 months 19/35 (54) 12/32 (37) Body acupuncture and auricular seed embedding versus auricular seed embedding (A3) 12/32 (37) 5/30 (17) Radmayr et al. [2001] 40 Laser acupuncture versus antidiuretic medication (C1) 1^3 months 6 months after treatment 13/20 (65) 15/20 (75) Ren [1987] 91 Needle acupuncture versus laser acupuncture (B6) ** Not stated 16/38 (42) 26/53 (49) Wang and Zhang [1999] 170 Acupuncture versus needle embedding (B7) 9^30 days 6 months 35/50 (70) 73/80 (91) Acupuncture versus catgut embedding (B8) 35/50 (70) 23/40 (58) Xiao and Zhang [2001] 84 Acupuncture and herbal medicine versus herbal medicine (A4) 3 weeks Not stated 40/43 (93) 31/41 (76) Xiao [1997] 42 Acupuncture versus vitamin injections over acupuncture points (B9)
- 49. ** Not stated 6/18 (33) 16/24 (66) Xu [1997] 45 Acupuncture versus moxibustion (B10) ** 6 months 12/15 (80) 22/30 (73) Acupuncture for Nocturnal Enuresis in Children 269 DISCUSSION Research from as early as 1958 identi¢ed spinal and per- ipheral nerves and their terminals dispersed within 5 mm of known acupuncture meridians. Nerves from such acupunc- ture points fed into the same area of the spine as certain vis- cera that have long been linked with such points [Cai, 1992]. More recently high concentrations of neuroendocrine trans- mitters and hormones have been identi¢ed at acupuncture points. Furthermore, needling or mechanical stimulation at these points induces release and spread of neurotransmitter substances [Omura, 1989; Kashiba and Ueda, 1991]. Addition of electrical stimulation during acupuncture induces endor- phin release that generates a more potent e¡ect on the con- centration of neuropeptides in the animal hippocampus and occipital cortex than manual acupuncture [Bucinskaite et al., 1994]. An autonomic response occurs during acupuncture, as evidenced by signi¢cantly reduction in average heart rate during treatment [Wu et al., 1999]. Functional magnetic imaging (fMRI) has recently been used to investigate neurobiological mechanisms underlying acupuncture therapy. Needling to a depth of 2 cm at ST36 (a point commonly utilized in the treatment of nocturnal enuresis) provoked activation of the hypothalamus, limbic system, and nucleus accumbens [Wu et al., 1999]. Both the
- 50. hypothalamus and the nucleus accumbens have descending projections and interconnections with periaqueductal gray matter (PAG), important in the modulation of bladder activ- ity. Control stimulation did not produce increased activity in the same deep structures, and needles left in situ without manipulation did not produce any fMRI signal changes [Wu et al., 1999; Hui et al., 2000]. Electroacupuncture con- sistently induced greater magnitude signal increases than manual acupuncture. Thus, there is sound evidence to accept that peripheral- ly applied acupuncture stimulates sensory nerves, increa- ses the release of neurotransmitters, neuropeptides, and hormones and increases cutaneous blood £ow and microcir- culation [Cai, 1992]. Neural impulses to the spinal cord are up-regulated and act on ascending pathways to the brain, creating the potential to modulate central nervous system functions [Shen, 2001]. Given such a theoretical framework it is encouraging that this systematic review provides some evidence in support of the e⁄cacy of acupuncture for nocturnal enuresis. This holds even though the criteria for success was strict, i.e., ‘‘cure.’’ Given that TCM routinely constitutes a number of modal- ities rather than individual techniques, ¢ndings from this review support the practice of acupuncture within a combi- nation therapy framework. Interpretation of results was limited by quality aspects of the studies. All the Chinese data comprised clinical reports and lacked patient sub-group classi¢cation, detailed methodology, and analysis. Post-treatment changes in blad- TABLE III. Jadad Trial Quality Scores
- 51. Author(s) and year of publication Randomization Double blinding Withdrawal or drop-out Total Jadad score (possible total ¼ 3) Ji and Zhou [2000] 0 0 0 0 Xiao and Zhang [2001] 0 0 0 0 Lu [2000] 0 0 0 0 Ren [1987] 0 0 0 0 Xiao [1997] 1 0 0 1 Li and Xue [1996] 1 0 0 1 Xu [1997] 0 0 0 0 Liu and Shen [1990] 1 0 0 1 Cai [1987] 0 0 0 0 Wang and Zhang [1999] 1 0 0 1 Radmayr et al. [2001] 1 0 0 1 Fig. 1. Comparison of acupuncture in combination with other therapy versus other therapy alone. 270 Bower et al. der storage, arousal, and detrusor activity were not report- ed, making it di⁄cult to associate gains with underlying phy- siological changes. Short post-treatment follow-up, being 6 months or less, was another limiting factor. It proved impossible to ascertain whether acupuncture was more e⁄cacious than standard treatment for nocturnal
- 52. enuresis since the comparative treatments were dissimilar (Fig. 2). A smaller di¡erence in treatment outcome would therefore be expected. In addition, some of the interventions that are compared to acupuncture have an unknown e⁄cacy, making it di⁄cult to interpret results. However, the results are highly heterogeneous, some show statistically signi¢cant results, and some of the 95% CI exclude each other. These ¢ndings do seem to give further support for an e⁄cacy of some forms of acupuncture, if not all. If every one of the compared acupunctures were ine¡ective, the large hetero- geneity would not have been observed. An alternative expla- nation could be di¡erence in the quality of the trials. Whilst acupuncture was signi¢cantly more e¡ective than either embedding seeds into the ear or saline injections over acupuncture points, needle embedding and vitamin in- jections over acupoints were signi¢cantly more useful than acupuncture. Clearly there is inconsistency since similar interventions produced such disparate results. Even though an investigator bias in favor of the test intervention would be expected when comparing novel treatments with standard practice, this is not substantiated. The evidence thus suggests that some forms of acupuncture are more e¡ective than other forms of either acupuncture or novel TCM modalities. No conclusions can be drawn as to which treatment forms are consistently superior for children with nocturnal enuresis. The comparison of western medicine’s current gold- standard treatment, the antidiuretic hormone vasopressin, with acupuncture, showed no signi¢cant di¡erence between the two modalities. The sample size might be considered in- adequate and the omission of sub-classi¢cation of children and a control group, study £aws. However, the lack of greater e⁄cacy for pharmacotherapy is a positive ¢nding for acupuncture.
- 53. Increasing scienti¢c understanding of acupuncture- induced physiological changes, coupled with signi¢cant posi- tive ¢ndings from this review, supports the need for further and rigorous high quality trials of the e⁄cacy of acupuncture for nocturnal enuresis. E¡ect of acupuncture on the known imbalances underlying western medicine understanding of nocturnal enuresis (small bladder capacity, poor arousal abil- ity, and nocturnal polyuria) would be clari¢ed with the in- clusion of initial urodynamic investigations, standardized Fig. 2. Comparison of conventional acupuncture and another acupuncture therapy. Fig. 3. Comparison of acupuncture with antidiuretic medication. Acupuncture for Nocturnal Enuresis in Children 271 symptom scoring, and sub-group classi¢cation. It would be helpful to stratify patients accordingly and thence compare acupuncture (�other TCM modalities) with the enuresis alarm and combination western medicine therapies. CONCLUSION This review provides tentative evidence for the e⁄cacy of acupuncture in the treatment of childhood nocturnal enur- esis. Due to the low methodological quality of studies, evi- dence to identify, which parameters of acupuncture work best, is lacking. More rigorous trials are clearly warranted. REFERENCES Berman BM. 2001. Clinical applications of acupuncture: An
- 54. overview of the evidence. J Alter Compl Med 7:S111^8. Bjorkstrom G, Hellstrom AL, Andersson S. 2000. Electro- acupuncture in the treatment of children with monosymptomatic nocturnal enuresis. Scand J Urol Nephrol 34:21^6. Bucinskaite V, Lundeberg T, Stenfors C, et al. 1994. E¡ects of electroacu- puncture and physical exercise on regional concentrations of neuropep- tides in rat brain. Brain Res 666:128^32. Cai ZM. 1987. Relation between the extent of distinctness of propagat- ed sensation along channels and therapeutic e¡ect of acupuncture on enuresis in Senegal patients. Acupunct Res 65^6. Cai W. 1992. Acupuncture and the nervous system. Am J Chin Med 20: 331^7. DerSimonian R, Laird N. 1986. Meta-analysis in clinical trials. Contr Clin Trials 7:177^88. Honjo H, Kawauchi A, Ukimura O, et al. 2002. Treatment of monosympto- matic nocturnal enuresis by acupuncture: A preliminary study. Int J Urol 9:672^6. Hui KS, Lui J, Makris N, et al. 2000. Acupuncture modulates
- 55. the limbic system and subcortical gray structures of the human brain: Evidence from fMRI studies in normal subjects. Hum Brain Map 9: 13^25. Jadad AR, Moore RA, Carroll D, et al. 1996. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Contr Clin Trials 17:1^12. Ji YX, Zhou LM. 2000. E⁄cacy of acupuncture in 138 patients with noctur- nal enuresis. Shangh J Acupunct Moxi 19:27. Kachan AT,Trubin MI, Skoromets AA, et al. 1993. Acupuncture re£exother- apy of neurogenic bladder dysfunction in children with enuresis. Zh Nevropatol Psikhiatr Im S S Korsakova 93:40^2. Kashiba H, Ueda Y. 1991. Acupuncture to the skin induces release of sub- stance P and calcitonin gene-related peptide from peripheral terminal of primary sensory neurons in the rat. Am J Chin Med 19:189^97. Li W, Xue YZ. 1996. E⁄cacy of catgut-embedding in the treatment of noc- turnal enuresis. Shang J Acupunct Moxi 15:23^4. Liu YX, Shen J. 1990. Comparative study of laser- magnetotherapy and acu- puncture in the treatment of nocturnal enuresis. Chin Acupunct
- 56. Moxi 5:19. Lu W. 2000. Comparative study on treatment of nocturnal enuresis by acu- puncture on head, body, and ear points. Chin Acupunct Moxi 20:25. Minni B, Capozza N, Creti G, et al. 1990. Bladder instability and enuresis treated by acupuncture and electro-therapeutics: Early urodynamic observations. Acupunct Electrother Res 15:19^25. OmuraY. 1989. Connections found between each Meridian and organ repre- sentation area of corresponding internal organs inside of the cerebral cortex. Acupunct Electrother Res Int J 14:155^86. Radmayr C, Schlager A, Studen M, et al. 2001. Prospective randomixed trial using laser acupuncture versus desmopressin in the treatment of noctur- nal enuresis. Eur Urol 40:201^5. Ren SZ. 1987. E⁄cacy of He-Ne laser acupuncture in the treatment of noc- turnal enuresis. Chin Acupunct Moxi 7:20. Serel TA, Perk H, Koyuncuoglu HR, et al. 2001. Acupuncture therapy in the management of persistent primary nocturnal enuresis. Scand J Urol Nephrol 35:40^3. Shen J. 2001. Research on the neurophysiological mechanisms
- 57. of acupunc- ture: Review of selected studies and methodological issues. J Alter Compl Med 7:S121^7. Tuzuner F, KecikY, Ozdemir S, et al. 1989. Electro-acupuncture in the treat- ment of enuresis nocturna. Acupunct Electrother Res 14:211^214. Wang JR, Zhang BF. 1999. Comparative study on treatment of nocturnal enuresis by needle-embedding, acupuncture, and catgut- embedding. Chin Acupunct Moxi 19:608. Wu MT, Hsieh JC, Xiong PC, et al. 1999. Central nervous pathway for acu- puncture stimulation: Localization of processing with functional MR imaging of the brain. Radiology 212:133^41. Xiao LF. 1997. E⁄cacy of VB1 and B12injection on acupoints in the treat- ment of nocturnal enuresis. Shang J Acupunct Moxi 16:22. Xiao L, Zhang SJ. 2001. Combination of traditional Chinese medicine and scalp acupuncture in 84 children with nocturnal enuresis. J Clin Acu- punct Moxi 17:14. Xu TB. 1997. The comparative study on the treatment of children’s enuresis by acupuncture and moxibustion. Acupunct Res 22:202.
- 58. Zhong MQ. 1986. Percussopunctator treatment of enuresis on the basis of di¡erential typing of symptoms. J Tradit Chin Med 3:171^5. 272 Bower et al. Antibiotics in Acute Bronchitis: A Meta-analysis Stephen Bent, MD, Sanjay Saint, MD, MPH, Eric Vittinghoff, PhD, Deborah Grady, MD, MPH PURPOSE: Most patients with acute bronchitis who seek med- ical care are treated with antibiotics, although the effectiveness of this intervention is uncertain. We performed a meta-analysis of randomized, controlled trials to estimate the effectiveness of antibiotics in the treatment of acute bronchitis. SUBJECTS AND METHODS: English-language studies pub- lished January 1966 to April 1998 were retrieved using MEDLINE, bibliographies, and consultation with experts. Only randomized trials that enrolled otherwise healthy patients with a diagnosis of acute bronchitis, used an antibiotic in the treat- ment group and a placebo in the control group, and provided sufficient data to calculate an effect size were included. RESULTS: We identified eight randomized controlled trials that satisfied all inclusion criteria. These studies used one of three antibiotics (erythromycin, doxycycline, trimethoprim/ sulfamethoxazole). The use of antibiotics decreased the dura- tion of cough and sputum production by approximately one- half day (summary effect size 0.21; 95% CI, 0.05 to 0.36). For specific symptoms, there were nonsignificant trends favoring the use of antibiotics: a decrease of 0.4 days of purulent sputum (95% CI, 20.1 to 0.8), a decrease of 0.5 days of cough (95% CI,
- 59. 20.1 to 1.1), and a decrease of 0.3 days lost from work (95% CI, 20.6 to 1.1). CONCLUSION: This meta-analysis suggests a small benefit from the use of the antibiotics erythromycin, doxycycline, or trimethoprim/sulfamethoxazole in the treatment of acute bron- chitis in otherwise healthy patients. As this small benefit must be weighed against the risk of side effects and the societal cost of increasing antibiotic resistance, we believe that the use of anti- biotics is not justified in these patients. Am J Med. 1999;107: 62– 67. q1999 by Excerpta Medica, Inc. A cute bronchitis is a common clinical disorder characterized by the acute onset of cough and sputum production in a patient with no history of chronic pulmonary disease and no evidence of pneumo- nia or sinusitis. This definition excludes patients with acute exacerbation of underlying pulmonary disorders, in whom a previous meta-analysis found that antibiotic use led to a small, statistically significant benefit (1). The effectiveness of antibiotics in patients with acute bronchi- tis remains uncertain, although the disorder is the tenth most common diagnosis seen by physicians in the United States, accounting for 10 million office visits annually (2). The etiology of acute bronchitis is unclear. Most stud- ies have identified viruses (adenovirus, rhinovirus, coro- navirus, influenza, parainfluenza, respiratory syncytial virus, and coxsackievirus) as the cause in the majority of patients (3–14). Atypical bacteria, including Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella spe- cies, have been reported to cause 5% to 25% of cases of acute bronchitis (15–17), and typical bacteria (Streptococ- cus pneumoniae, Haemophilus influenzae, Branhamella
- 60. catarrhalis) have been recovered from the sputum in 7% to 44% of patients (8,18,19). However, the importance of positive bacterial cultures from sputum is not known, because many of these pathogens are part of the oropha- ryngeal flora (3,9,20 –22). Recent evidence suggests that some bronchitis in adults may be caused by Bordetella pertussis and parapertussis, which are better known for their role in causing whooping cough in children (23). The majority of patients diagnosed with acute bronchi- tis in the United States are treated with antibiotics (24 – 27). In a nationwide survey of .1,500 physicians, Gonza- les et al (25) found that two-thirds of patients without underlying lung disease who were diagnosed with acute bronchitis were treated with antibiotics. In another sur- vey, 75% of children with a diagnosis of acute bronchitis were given a prescription for antibiotics (26). Although antibiotics are often used in the treatment of acute bronchitis, their efficacy is uncertain. Clinical trials examining this issue have yielded conflicting results (28 – 37), and qualitative reviews are similarly inconclusive (7,9,17,38,39). Widespread antibiotic use carries a sub- stantial cost, puts patients at risk for medication side ef- fects, and promotes antibiotic resistance. To clarify the optimal treatment of this disorder, we performed a meta-analysis to determine whether antibi- otics were beneficial in patients with acute bronchitis. Using explicit inclusion and exclusion criteria and ac- cepted quantitative methods (40 – 42), a meta-analysis provides summary estimates of effectiveness that may clarify the disparate results of previous trials (43). METHODS
- 61. Literature Review The literature review began with a computerized MEDLINE search using the subheading “bronchitis, drug From the Departments of Medicine (SB, SS, DG) and Epidemiology and Biostatistics (DG, EV), University of California, San Francisco, School of Medicine, San Francisco, California; Medical Service, San Francisco Veterans Affairs Medical Center (SB, SS, DG), San Francisco, Califor- nia. Dr Saint is now affiliated with the University of Michigan, Division of General Medicine, Department of Internal Medicine. Requests for reprints should be addressed to Stephen Bent, MD, Gen- eral Internal Medicine Section, San Francisco Veterans Affairs Medical Center 111A1, 4150 Clement Street, San Francisco, California 94121. Manuscript submitted August 5, 1998, and accepted in revised form February 24, 1999. 62 q1999 by Excerpta Medica, Inc. 0002-9343/99/$–see front matter All rights reserved. PII S0002-9343(99)00167-9 therapy” and the term “xs acute disease,” and included English-language articles published between January
- 62. 1966 and April 1998. The reference lists of all retrieved articles were scanned, and experts were consulted to iden- tify potential trials not identified in the MEDLINE search. Inclusion criteria consisted of the following: random- ized trials using an antibiotic in the treatment group and a placebo in the control group; subjects with acute bron- chitis, no history of chronic lung disease, and pneumonia excluded by chest radiograph or clinical exam; therapy for at least 5 days; and the presentation of sufficient data to calculate the difference in efficacy between the treat- ment and the placebo as a continuous variable. Studies were excluded if they were nonexperimental in design or if they compared one antibiotic with another without a placebo arm. For each study, two authors independently abstracted the author, journal title, year of publication, sample size, average age of subjects, antibiotic regimen used, major outcome measure(s), and the inclusion and exclusion cri- teria. Discrepancies in the abstracted data were resolved by consensus. Analysis The eight eligible studies did not use a common outcome measure. When several outcomes were available from one study, we chose “days of sputum production” as the main outcome, because this symptom is most character- istic of the disease (4). For studies that did not include the outcome “days of sputum production,” we chose the out- come in the study that was the most clinically similar (sputum production score, cough amount score). We transformed each outcome into units of standard devia- tion, thus giving a comparable effect size for different outcomes. The study-specific effect size was the differ- ence in the mean outcome for the antibiotic and placebo
- 63. groups, divided by the pooled standard deviation of the outcome measure in that study. The summary effect size across studies was calculated as a weighted average of the study-specific effect sizes, with weights equal to the in- verse of the estimated variance. The significance of the summary effect size, standardized by its estimated vari- ance, was assessed by comparing it with the standard nor- mal distribution. A test for heterogeneity was calculated by comparing the weighted average of the squared differ- ences between summary and study-specific effect sizes with an appropriate X2 distribution, with the same weights being used. These calculations used standard for- mulas (44), which assume that the outcomes are nor- mally distributed and the sample sizes are approximately equal in the antibiotic and placebo groups. We also calculated summary mean differences for all outcomes reported by four or more studies. The sum- mary measure was the weighted average of the difference between the antibiotic and placebo groups in the mean outcome measure for each study. Weights were given by the inverse of the variance of each mean difference, esti- mated using the pooled standard deviation for each study. Tests of the significance of the observed summary mean differences and of heterogeneity were also per- formed (44). We examined the potential for publication bias using the correlation between the number of subjects and the effect size in each study. If small studies with negative results were less likely to be published, then the correla- tion between number of subjects and effect size would be large. If there was not any publication bias, then there should not be a significant correlation between the num- ber of subjects and the effect size.
- 64. RESULTS Our search identified 203 reports, including 10 random- ized, placebo-controlled trials of antibiotics for the treat- ment of acute bronchitis (28 –37). Two (28,31) of these studies had to be excluded because insufficient data were presented in the original articles, and attempts to retrieve the necessary data from the authors were unsuccessful. The remaining eight trials, all of which used one of three antibiotics (erythromycin, doxycycline, trimethoprim/ sulfamethoxazole), were included in the meta-analysis. Reasons for exclusion are listed in Table 1. The character- istics of the 10 randomized controlled trials, including the two that were excluded because of insufficient data, are shown in Table 2. The overall summary effect size was 0.21 (95% CI, 0.05 to 0.36) indicating a small (about one-fifth of a standard deviation), statistically significant benefit from the use of antibiotics (Figure), equivalent to approximately one half day less of cough and sputum production. Three outcomes were reported by at least four studies (Table 3). Although each of these results favor antibiotics, none was statistically significant. For days of purulent Table 1. Reasons for Exclusion of Reports Retrieved from Lit- erature Search Reason for Exclusion Number of Reports Not original data 74
- 65. No control group 87 Main intervention was not antibiotic therapy 16 Patients with COPD were included 11 Main intervention was prophylaxis 1 Subjects had another infectious disorder (sinusitis, bronchiolitis) 4 Insufficient data presented 2 Total excluded 195 COPD 5 chronic obstructive pulmonary disease. Antibiotics in Acute Bronchitis/Bent et al July 1999 THE AMERICAN JOURNAL OF MEDICINEt Volume 107 63 sputum, the summary mean difference was 0.4 (95% CI, 20.1 to 0.8); the mean difference was 0.5 (95% CI, 20.1 to 1.1) for days of cough and 0.3 (95% CI, 20.6 to 1.1) for days lost from work. The effect of antibiotic treatment on days lost from work was very small, and unlike days of cough and sputum production, did not approach statis- tical significance. A test for heterogeneity was not significant for the overall summary effect size (P 5 0.37) or for days of spu- tum production (P 5 0.50), suggesting that these results are homogenous and can be combined. A test for heter- ogeneity was significant for the summary mean difference for days lost from work (P 5 0.03) and days of cough
- 66. Table 2. Randomized Trials of Antibiotics in Acute Bronchitis First Author, Year (reference) No. of Subjects Antibiotic Main Outcome Measure Study Result (95% CI)* Standardized Effect Size (95% CI)† Howie, 1970 (31) 836 Demethyl-chlortetracycline Average days of purulent spit 0.3‡ Not available‡ Stott, 1976 (33) 207 Doxycycline Days of yellow spit 0.6 (20.2 to 1.4) 0.20 (20.08 to 0.48) Franks, 1984 (30) 54 Trimethoprim/sulfamethoxazole Cough amount score 0.2 (20.2 to 0.6)§ 0.25 (20.30 to 0.79) Williamson, 1984 (34) 69 Doxycycline Days of purulent sputum
- 67. 20.2 (21.2 to 0.8) 20.09 (20.57 to 0.38) Brickfield, 1986 (28) 50 Erythromycin Sputum production score 0.2‡¶ Not available‡ Dunlay, 1987 (29) 45 Erythromycin Sputum production score on day 10 0.5 (0.1 to 0.9)# 0.80 (0.20 to 1.41) Scherl, 1987 (32) 31 Doxycycline Days of sputum 1.9 (20.2 to 4.0) 0.64 (20.08 to 1.36) Verheij, 1994 (35) 140 Doxycycline Days of productive cough 0.5 (20.4 to 1.4) 0.18 (20.15 to 0.52) Hueston, 1994 (36) 23 Erythromycin Days of productive cough 20.4 (22.4 to 1.6) 20.21 (21.14 to 0.72) King, 1996 (37) 91 Erythromycin Days of sputum production 0.7 (21.3 to 2.7) 0.14 (20.27 to 0.55)
- 68. * Result is the mean in the antibiotic group minus the mean in the placebo group for the main outcome measure. A positive result indicates a benefit from antibiotics. A negative result indicates a benefit from placebo. † Effect size is the difference between the mean outcome in the antibiotic and placebo groups divided by the pooled standard deviation. ‡ These studies did not provide data that allowed calculation of a confidence interval or a continuous outcome measure, and therefore could not be included in the overall summary effect size. § Cough amount score was a patient-reported score on a severity scale of 1 to 3. ¶ Sputum production score was a patient-reported score on a severity scale of 1 to 4. # Sputum production score was a patient-reported score on a severity scale of 1 to 5. CI 5 confidence interval. Figure. Effect sizes and summary overall estimate. Effect size is the difference between the mean outcome in the antibiotic and placebo groups divided by the pooled standard deviation. Hor- izontal lines denote 95% confidence intervals. Dots represent point estimates. Table 3. Summary Mean Differences between Antibiotic and Placebo Groups Outcome Measure (reference) Summary Mean Difference (95% CI)* Days of purulent sputum (6 trials)
- 69. (32–37) 0.4 days (20.1–0.8) Days of cough (4 trials) (32–35) 0.5 days (20.1–1.1)† Time off work (6 trials) (32–37) 0.3 days (20.6–1.1)† * Summary mean difference is the weighted average of the difference between the antibiotic and placebo groups in the mean outcome mea- sure for each study. † A test of heterogeneity was statistically significant. CI 5 confidence interval. Antibiotics in Acute Bronchitis/Bent et al 64 July 1999 THE AMERICAN JOURNAL OF MEDICINEt Volume 107 (P 5 0.05), suggesting that these outcomes may have been derived from studies that used different methods. There was no correlation between study size and overall effect size (r 5 20.13, P 5 0.75). DISCUSSION Randomized controlled trials evaluating the efficacy of antibiotics in acute bronchitis have had inconsistent re- sults. Of the eight trials included in our meta-analysis, four showed no benefit from the use of antibiotics (32– 34,36), whereas four reported a benefit (29,30,35,37). Part of the discrepancy may be because studies used dif-
- 70. ferent outcome measures, some of which are of uncertain clinical importance. For example, the outcome measures in one trial that reported a statistically significant benefit from antibiotics included a reduction in mean tempera- ture from 37.38C to 36.98C and a reduction in the use of antihistamines (30). Because the published trials used several outcome measures, we used the standardized effect size, expressed in units of standard deviation, to quantitate the overall effect of antibiotic therapy. We chose the outcome that is most characteristic of acute bronchitis (days of sputum production) in the six studies where it was available, and we used the most similar outcome in the two other stud- ies (cough amount score, sputum production score). We found a small, statistically significant benefit to the use of antibiotics in patients with acute bronchitis approxi- mately equal to one-fifth of a standard deviation unit. To relate the observed benefit in the summary effect size to clinical variables, we also calculated summary mean dif- ferences for all outcomes that were reported by at least four trials (duration of sputum production, duration of cough, and days lost from work), all of which showed small, nonsignificant trends favoring the use of antibiot- ics. Our meta-analysis suggests that patients with acute bronchitis who are treated with antibiotics have a reduc- tion in the duration of cough and sputum production of approximately one half day. Our results should be interpreted with caution. As with all meta-analyses, we assumed that the individual trials are sufficiently similar to provide a meaningful summary. The studies did have several important differences. They took place in different geographic locations, used three different antibiotics (erythromycin, doxycycline, tri- methoprim/sulfamethoxazole), and were conducted
- 71. during a 20-year period. However, despite these differ- ences, statistical tests for heterogeneity did not show dif- ferences between studies for the main outcome, or for the outcome of sputum production. Although different anti- biotics were used, all groups were treated for at least 5 days, and the spectrum of organisms covered by the var- ious antibiotics was similar. We identified 10 randomized controlled trials in our literature review. Results from two of these trials could not be included because insufficient data were reported (28,31). Both of these trials showed no benefit from the use of antibiotics. Thus, their exclusion tended to bias our results in favor of antibiotics. In addition, the summary effect size may have been overestimated if publication bias made it more likely that studies showing benefit were published, whereas those showing no benefit were not. If there was publication bias, small studies with negative findings should have been unlikely to be published, whereas small studies with positive findings should have been more likely to be published, leading to a correlation between study size and effect size. We found no such correlation. We used similar methodology to an earlier meta-anal- ysis that examined the effect of antibiotics in patients with acute exacerbations of chronic obstructive pulmonary disease (1). That study reported a summary effect size of 0.22 (95% CI, 0.10 to 0.34), also indicating a small, sta- tistically significant benefit from the use of antibiotics. Patients who were treated with antibiotics had a modest improvement in peak expiratory flow of approximately 11 L/min compared with those treated with placebo. Al- though the magnitude of benefit from antibiotic treat- ment in that meta-analysis is similar to that in the current meta-analysis, such a benefit may be more important for
- 72. a patient with underlying lung disease who has less func- tional reserve. The costs of widespread antibiotic use are great for both patients and society. They include prescription costs, medication side effects, and an increase in antibi- otic resistance. Several studies have shown that wide- spread antibiotic use leads to the development of resistant organisms (45– 47). Antibiotic use for acute bronchitis constitutes a substantial portion of all antibiotic use in the United States, accounting for 9% of all prescriptions writ- ten for children (26). Furthermore, side effects of antibi- otics used for acute bronchitis are common, occurring in 10% to 36% of patients (28 –31,33,35,37). The practice of routinely giving antibiotics for acute bronchitis encour- ages patients to expect antibiotics for subsequent epi- sodes (48), which adds to the cycle of medication costs, side effects, and antibiotic resistance. We believe that there should be a clear, substantial benefit to antibiotics to justify these costs. Some authors have suggested that certain subgroups of patients with acute bronchitis may benefit from antibiot- ics (9,35,39). In a study of 140 patients randomly assigned to treatment with doxycycline or placebo, Verheij et al (35) reported that doxycycline resulted in clinical benefit among patients older than 55 years and in those who felt ill at study entry. However, approximately 30% of the patients in that study had abnormalities on lung auscul- tation and therefore may have had conditions such as Antibiotics in Acute Bronchitis/Bent et al July 1999 THE AMERICAN JOURNAL OF MEDICINEt Volume 107 65
- 73. pneumonia that would show a large benefit from antibi- otic treatment (49). Others have suggested treating pa- tients who test positive for Mycoplasma pneumoniae or Chlamydia pneumoniae (39), although there is no evi- dence from randomized trials to support this practice. In a randomized trial using erythromycin to treat acute bronchitis, King et al (37) found no difference in out- comes between patients who tested positive and those who tested negative for Mycoplasma pneumoniae. More research is needed to determine if there are subgroups of patients who are likely to have a substantial benefit from treatment with antibiotics. The studies included in this meta-analysis examined the effect of one of three different antibiotics (erythromy- cin, doxycycline, trimethoprim/sulfamethoxazole). None of the studies used one of the newer macrolide or floro- quinolone antibiotics. We are not aware of any random- ized, placebo-controlled trials of these agents in adults with acute bronchitis. Future studies should determine the risks and benefits associated with use of these newer antibiotics. In summary, we found a statistically significant benefit from the use of antibiotics in acute bronchitis. Treatment reduced the duration of cough and sputum production by approximately one half day. The decision to use anti- biotics for the treatment of adults with acute bronchitis must be weighed against the costs associated with wide- spread use of these agents. In healthy patients with acute bronchitis who have no evidence of chronic pulmonary disease, we believe that the small benefit associated with antibiotic treatment does not outweigh the risk of side effects and the increase in antibiotic resistance.
- 74. Note Added in Proof: After this paper was submitted, a meta-analysis on a similar topic was published: Smucny JJ, Becker LA, Glazier RH, McIsaac W. Are antibiotics effective treatment for acute bronchitis? A meta-analysis. J Fam Pract. 1998;47:453– 460. REFERENCES 1. Saint S, Bent S, Vittinghoff E, Grady D. Antibiotics in chronic ob- structive pulmonary disease exacerbations: a meta-analysis. JAMA. 1995;273:957–960. 2. Woodwell DA, Schappert SM. National Ambulatory Medical Care Survey: 1993 summary. Advance Data. 1995;270:1–20. 3. Billas A. Lower respiratory tract infections. Prim Care. 1990;17: 811– 824. 4. Chow AW, Hall CB, Klein JO, Kammer RB, Meyer RD, Remington JS. Evaluation of new anti-infective drugs for the treatment of re- spiratory tract infections. Infectious Diseases Society of America and the Food and Drug Administration. Clin Infect Dis. 1992;15: S62–S88. 5. Hitt JA, Gerding DN. Sputum antimicrobial levels and clinical out- come in bronchitis. Semin Respir Infect. 1991;6:122–128.
- 75. 6. Hosker HS, Jones GM, Hawkey P. Management of community ac- quired lower respiratory tract infection. BMJ. 1994;308:701– 705. 7. Gleckman RA. Bronchial infections: acute bronchitis and acute ex- acerbation of chronic bronchitis. Compr Ther. 1987;13:44 – 48. 8. Boldy DA, Skidmore SJ, Ayres JG. Acute bronchitis in the community: clinical features, infective factors, changes in pulmo- nary function and bronchial reactivity to histamine. Respir Med. 1990;84:377–385. 9. Rodnick JE, Gude JK. The use of antibiotics in acute bronchitis and acute exacerbations of chronic bronchitis. West J Med. 1988;149: 347–351. 10. Trigg CJ, Davies RJ. Antibiotic prescribing for bronchitis: time for a change? Respir Med. 1994;88:161–163. 11. Garibaldi RA. Epidemiology of community-acquired respiratory tract infections in adults. Incidence, etiology, and impact. Am J Med. 1985;78:32–37. 12. Dunlay J, Reinhardt R. Clinical features and treatment of acute bronchitis. J Fam Pract. 1984;18:719 –722. 13. Vogel F. A guide to the treatment of lower respiratory tract