Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine
•
2 likes•166 views

Jonathan Corren, MD, discusses asthma management in this CME activity titled "Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine." For the full presentation, downloadable infographics, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2It37Pk. CME credit will be available until June 3, 2019.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine
Similar to Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine
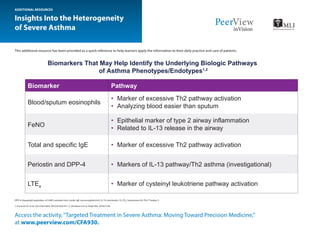
- 1. This additional resource has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Insights Into the Heterogeneity of Severe Asthma DPP-4: dipeptidyl peptidase-4; FeNO: exhaled nitric oxide; IgE: immunoglobulin E; IL-13: interleukin 13; LTE4 : leukotriene E4; Th2: T helper 2. 1. Erzurum SC et al. Clin Chest Med. 2012;33:459-471. 2. Shiobara S et al. Respir Res. 2016;17:28. ADDITIONAL RESOURCES Access the activity,“Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine,” at www.peerview.com/CFA930. Blood/sputum eosinophils • Marker of excessive Th2 pathway activation • Analyzing blood easier than sputum • Epithelial marker of type 2 airway inflammation • Related to IL-13 release in the airway • Marker of excessive Th2 pathway activation • Markers of IL-13 pathway/Th2 asthma (investigational) • Marker of cysteinyl leukotriene pathway activation FeNO Total and specific IgE Periostin and DPP-4 LTE4 Biomarker Biomarkers That May Help Identify the Underlying Biologic Pathways of Asthma Phenotypes/Endotypes1,2 Pathway
- 2. Access the activity,“Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine,”at www.peerview.com/CFA930. New Horizons in the Treatment of Severe Asthma This additional resource has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. ADDITIONAL RESOURCES • Similar results observed for the 200-mg Q2W dose group • Extent of patient response correlated with blood eosinophils and other markers—less activity was observed in patients with <150 eosinophils/mcL QUEST Study: Improvements With Dupilumab 300 mg Q2W Clinical Trial Data for Emerging Treatment Options: Dupilumab5-9 a P < .001 vs placebo for all groups. Overall rates of AEs, deaths, infections, conjunctivitis, herpes, and discontinuations comparable with placebo Injection-Site Reactions Dupilumab 300 mg Q2W: 18.4% Matched placebo: 10.3% Overall Population ≥300 Eosinophils/mcL 1,795 Adults 107 Adolescents 9 18 0 5 10 15 20 25 30 FEV1 at 12 Wk, %a 130 mL 240 mL Exacerbations at 52 Wk, %a -46 -67 -60 -80 -40 -20 0 Parameter Mepolizumab Reslizumab Benralizumab Patient age ≥12 y ≥18 y ≥12 y Route SubQ IV SubQ Dosing Q4W Q4W Adjusted by weight Q4W for first 3 doses, then Q8W Eosinophils ≥150/mcL ≥400/mcL ≥150/mcL Which Anti–IL-5 to Choose?1-4 No head-to-head studies • Rates of AEs, including infections, conjunctivitis, and herpes, comparable between groups • Injection-site reactions more common in dupilumab group (9%) vs placebo group (4%) • Increase in eosinophil counts more frequent in dupilumab group (14%) vs placebo group (1%); mostly mild and resolved spontaneously Improvements in lung function and exacerbations observed despite decreased OCS use Outcomes Overall Population Patients With ≥300 Eosinophils/mcL Dupilumab 300 mg Q2W P vs Placebo Dupilumab 300 mg Q2W P vs Placebo $ Maintenance OCS use 70% < .0001 80% .0001 (nominal) $ Exacerbations 59% < .0001 71% Not listed # FEV1 15% (220 mL) .0007 25% (320 mL) .0049 (nominal) LIBERTY ASTHMA VENTURE, 24-Wk Phase 3 Data, 210 Patients Requiring Oral Steroids
- 3. Access the activity,“Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine,”at www.peerview.com/CFA930. New Horizons in the Treatment of Severe Asthma This additional resource has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. ADDITIONAL RESOURCES • Significantly improved annualized rate of asthma exacerbations at wk 52 in all dose groups • Significantly improved prebronchodilator FEV1 at wk 52 in all dose groups • Greater proportion of patients in tezepelumab groups either well or partially controlled at wk 52 • 2 patients in medium-dose group, 3 in high-dose group, and 1 in placebo group discontinued because of AEs Subpopulation Analysis Blood Eosinophil Count, cells/mcL Clinical Trial Data for Emerging Treatment Options: Tezepelumab10-13 0 0.2 0.4 0.6 0.8 1.0 FeNO, ppb Th2 Status HighLow≥24<24≥250<250 AnnualizedRateofExacerbations, Events/Patient-Year P = .03 P = .001 P = .001 P = .02 P = .006 P = .006 P = .03 P < .001 P < .001 P < .001 P = .008 P < .001 P = .004 P = .005 P = .02 n Placebo n Low-dose tezepelumab (70 mg Q4W) n Medium-dose tezepelumab (210 mg Q4W) n High-dose tezepelumab (280 mg Q2W) Significantly $ eosinophilic inflammation in sputum and bronchial submucosa in patients with persistent moderate to severe asthma and sputum eosinophilia Significantly improved AQLQ(S) scores, post-bronchodilator FEV1 , and functional residual capacity in all patients, and ACQ-7 scores in the predefined subgroup of patients who had uncontrolled asthma at baseline Favorable safety profile, with no deaths or serious AEs reported Clinical Trial Data for Emerging Treatment Options: Fevipiprant14-19 16 8 4 2 1 0.5 1260 18 Treatment Washout Time, wk FoldReductioninSputum EosinophilCount Fevipiprant Placebo P = .0014 P = .0077 P = .92
- 4. Access the activity,“Targeted Treatment in Severe Asthma: Moving Toward Precision Medicine,”at www.peerview.com/CFA930. New Horizons in the Treatment of Severe Asthma This additional resource has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. ACQ-7: Asthma Control Questionnaire–7; AEs: adverse events; AQLQ(S): standardized Asthma Quality of Life Questionnaire; BID: twice daily; FeNO: exhaled nitric oxide; FEV1 : forced expiratory volume in 1 second; IL-5: interleukin 5; OCS: oral corticosteroids; QD: once daily; QxW: every x weeks; Th2: T helper 2. 1. Maselli D et al. J Asthma Allergy. 2016;9:155-162. 2. Nucala (mepolizumab) Prescribing Information. http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125526Orig1s000Lbl.pdf. Accessed March 5, 2018. 3. Cinqair (reslizumab) Prescribing Information. http://cinqair.com/pdf/PrescribingInformation.pdf. Accessed May 4, 2018. 4. Fasenra (benralizumab) Prescribing Information. https://www.azpicentral.com/fasenra/fasenra_pi.pdf. Accessed March 5, 2018. 5. https://www.prnewswire.com/news-releases/fda-to-review-dupixent-dupilumab-as-potential- treatment-for-moderate-to-severe-asthma-300607094.html. Accessed May 4, 2018. 6. https://www.prnewswire.com/news-releases/regeneron-and-sanofi-announce-positive-dupilumab- topline-results-from-phase-3-trial-in-uncontrolled-persistent-asthma-300516839.html. Accessed May 4, 2018. 7. https://globenewswire.com/news-release/2017/10/31/1169458/0/en/ Sanofi-Dupilumab-Significantly-Reduced-Steroid-Use-Asthma-Attacks-and-Improved-Lung-Function-in-a-Phase-3-Study-of-People-with-Severe-Steroid-Dependent-Asthma.html. Accessed May 4, 2018. 8. Castro M et al. N Engl J Med. May 21, 2018. [Epub ahead of print]. 9. Rabe KF et al. N Engl J Med. May 21, 2018. [Epub ahead of print]. 10. https://www.clinicaltrials.gov/ct2/show/ NCT03347279. Accessed May 4, 2018. 11. Corren J et al. N Engl J Med. 2017;377:936-946. 12. Corren J et al. American Academy of Allergy, Asthma and Immunology and World Allergy Organization 2018 Joint Congress (AAAAI/WAO 2018). Abstract 257. 13. Corren J et al. American Thoracic Society Conference 2018 (ATS 2018). Abstract A5962. 14. https://www.clinicaltrials.gov/ct2/show/ NCT03052517. Accessed May 4, 2018. 15. https://www.clinicaltrials.gov/ct2/show/NCT02563067. Accessed May 4, 2018. 16. https://www.clinicaltrials.gov/ct2/show/NCT02555683. Accessed May 4, 2018. 17. Bateman ED et al. Eur Respir J. 2017;50:1700670. 18. Kerwin EM et al. ATS 2018. Abstract 1408. 19. Gonem S et al. Lancet Respir Med. 2016;4:699-707. ADDITIONAL RESOURCES a P values are not adjusted for multiplicity. Change in FEV1 After 12 Wk of Treatment Treatment Group Difference vs Placebo, L (95% CI) Pa Fevipiprant 1 mg QD 0.075 (-0.048 to 0.198) .2296 Fevipiprant 3 mg QD 0.087 (-0.035 to 0.209) .1609 Fevipiprant 10 mg QD 0.002 (-0.125 to 0.129) .9760 Fevipiprant 30 mg QD 0.091 (-0.027 to 0.210) .1311 Fevipiprant 50 mg QD 0.052 (-0.071 to 0.175) .4072 Fevipiprant 75 mg QD 0.111 (-0.007 to 0.230) .0652 Fevipiprant 150 mg QD 0.164 (0.044 to 0.285) .0075 Fevipiprant 300 mg QD 0.120 (0.003 to 0.237) .0442 Fevipiprant 450 mg QD 0.077 (-0.012 to 0.167) .0901 Fevipiprant 2 mg BID -0.014 (-0.135 to 0.107) .8230 Fevipiprant 25 mg BID 0.145 (0.030 to 0.260) .0133 Fevipiprant 75 mg BID 0.179 (0.052 to 0.307) .0059 Fevipiprant 150 mg BID 0.064 (-0.054 to 0.181) .2871 Montelukast 10 mg 0.134 (0.045 to 0.222) .0033 Significant improvement in primary endpoint of change in predose FEV1 at wk 12 (P = .0035) with a maximum model-averaged difference to placebo of 0.112 L Fevipiprant Phase 2 Data in Uncontrolled Allergic Asthma