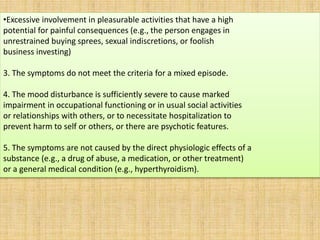
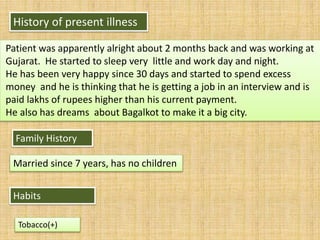
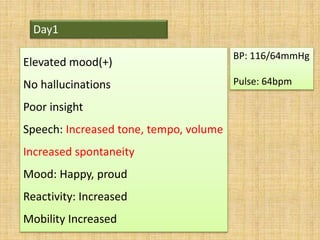
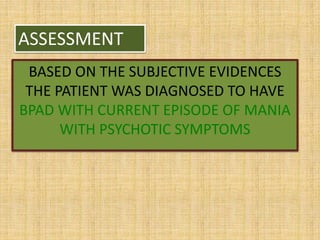
BPAD- CURRENT EPISODE OF MANIA WITH PSYCHOTIC SYMPTOMS
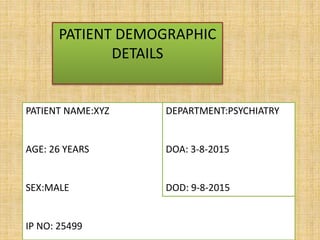
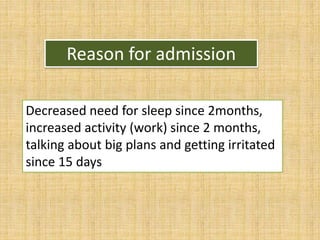
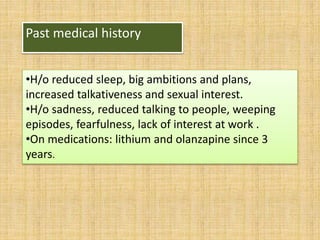
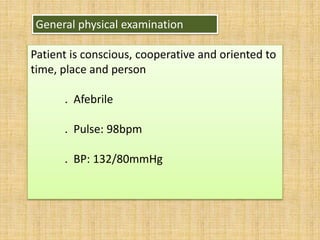
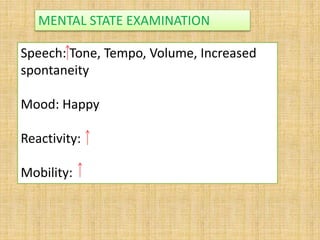
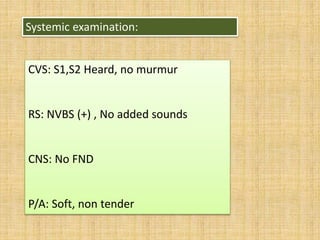
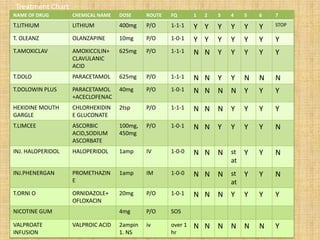
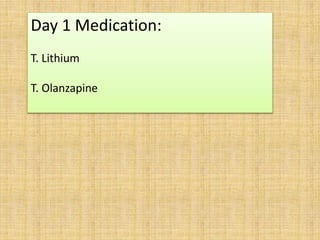
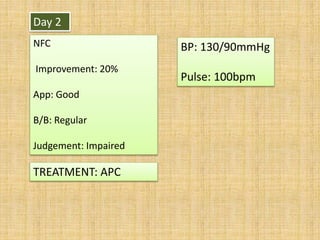
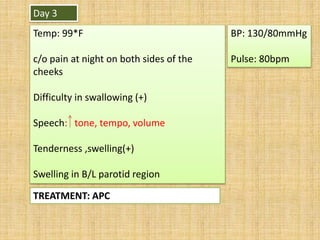
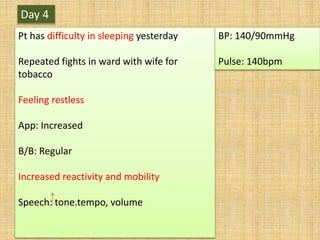
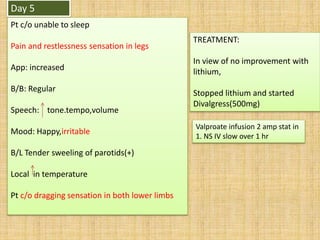
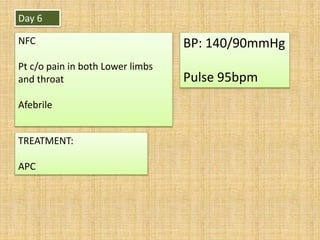
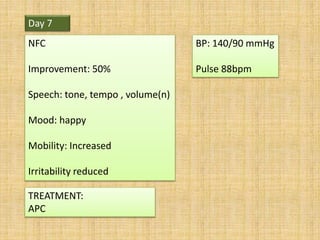
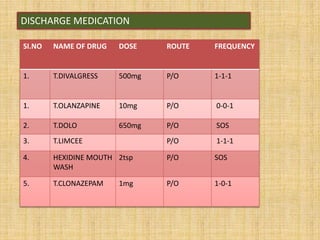
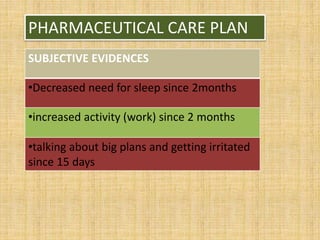
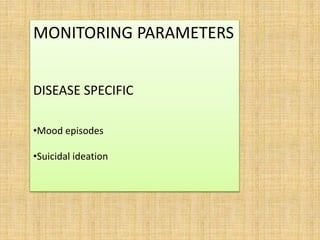
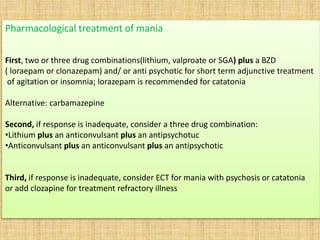
The patient, a 26-year-old male, presented with decreased need for sleep, increased activity and talkativeness, irritability, and psychotic symptoms over the past 2 months. He was diagnosed with bipolar affective disorder with a current manic episode with psychotic features. He was treated with lithium, olanzapine, and other medications but showed limited improvement. His treatment was changed to include divalproex and clonazepam in addition to olanzapine, which led to 50% improvement in his symptoms over one week.





























![Bipolar disorders [2002]](https://cdn.slidesharecdn.com/ss_thumbnails/bipolardisorders-170814010745-thumbnail.jpg?width=640&height=640&fit=bounds)








![Mood disorders [affective disorders]](https://cdn.slidesharecdn.com/ss_thumbnails/ayush2-200912131153-thumbnail.jpg?width=640&height=640&fit=bounds)























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





