Case Review #46: 56 year old female with Adult Idiopathic Scoliosis and Burst Fracture
•
0 likes•610 views

56 year old female with Idiopathic Scoliosis, status post burst fracture, presented with junctional kyphosis. Dr. Pashman treated the patient with a posterior spinal fusion from T2-pelvis. Spinal curvature was a KIM/SRP Classification 3.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Case Review #46: 56 year old female with Adult Idiopathic Scoliosis and Burst Fracture
Similar to Case Review #46: 56 year old female with Adult Idiopathic Scoliosis and Burst Fracture (20)
More from Robert Pashman
More from Robert Pashman (13)
Recently uploaded
Recently uploaded (20)
Case Review #46: 56 year old female with Adult Idiopathic Scoliosis and Burst Fracture
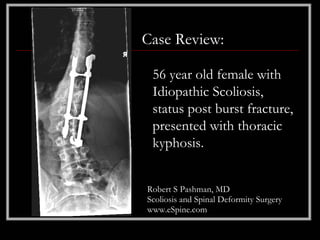
- 1. Case Review: 56 year old female with Idiopathic Scoliosis, status post burst fracture, presented with thoracic kyphosis. Robert S Pashman, MD Scoliosis and Spinal Deformity Surgery www.eSpine.com
- 2. Patient History • 56-year-old female • Status post burst fracture from an airplane crash greater than 15 years ago, pre-existing diagnosis of Idiopathic Scoliosis • Now superimposed burst fracture caused spinal cord compression and was treated with thoraco-abdominal vertebrectomy strut grafting followed by posterior instrumentation with Cottrell Dubois instrumentation • The patient had the instrumentation in situ but now is developing a thoracic kyphosis, subjacent degeneration with forward and coronal plane decompensation causing significant pain, radicular and low back. • Failed conservative therapy.
- 4. Indications for Surgery 1. Status post burst fracture, thoracolumbar junction. 2. Status post anterior spinal fusion with vertebrectomy strut graft, T11-L1. 3. Status post posterior instrumented fusion with CD (Cottrell Dubois) hook rod construct thoracolumbar spine. 4. History of adolescent/adult idiopathic scoliosis. 5. Now with proximal junctional kyphosis and subjacent degeneration with coronal and sagittal plane decompensation. 6. Low back radicular pain, failed conservative therapy. 7. Co-morbidity of von Willebrand's disease.
- 5. Surgical Strategy • Segmental spinal instrumentation, thoracic to sacral pelvis. This is an 18 level segmental spinal instrumentation using stainless steel 5.5 pedicle screw rod construct with sacral pelvic fixation. • Posterior spinal fusion, T2 to sacral pelvis using locally harvested autogenous bone in RH BMP. • Multilevel Smith-Peterson osteotomy, T4 to L4. This is a 16 level Smith-Peterson osteotomy for mobilization of the spine for posterior base only, coronal and sagittal plane correction. • Laminectomy, L1 to L4, for decompression and mobilization of subjacent spine with Smith-Peterson osteotomy under the microscope loupe magnification. • Intraoperative SSEPs. • Intraoperative fluoroscopy.
- 6. Post-op Films The patient is well balanced in the coronal and sagittal planes.