2. Scoliosis
Derived from the Greek word meaning
“Crooked”
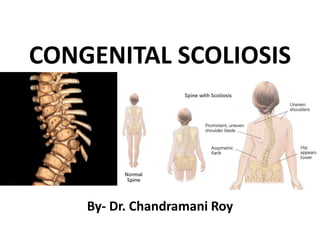
Definition – Lateral deviation of the normal
vertical line of the spine.
Lateral curvature of spine is also associated with
the rotation of vertebrae producing a three
dimensional deformity of the spine which
occurs in sagittal, frontal and coronal planes.
3. Etiological classification
1. Non structural Scoliosis
A. Postural scoliosis-
-Notated on later part of first decade.
-Curves are slight.
-Disappears on lying down/bending forward.
B. Compensatory Scoliosis-
- due to limb length discrepancies
- pelvic tilts on shorter side
- disappears on sitting
4. 2. Transient structural scoliosis-
A. Sciatic Scoliosis- unilateral painful spasm
of paraspinal muscles
B. Inflammatory scoliosis- Perinepheric
abscess
C. Hysterical scoliosis
5. 3. Structural scoliosis-
A. Idiopathic scoliosis-
a. Infantile type- birth to 3 yrs
b. Juvenile type- 4 to 9 yrs
c. Adolescent type- 10 to 20 yrs
B. Congenital Scoliosis
a. Vertebral.
b. Extravertebral- e.g. Congenital rib fusion
c. Neuromuscular Scoliosis-
i - Neuropathic- e.g. Polio, CP, Syringomyelia
ii- Myopathic- e.g. Muscular dystrophy, AMC,
Myotonic dystrophia
6. C. Developmental Scoliosis-
a. Congenital- Marfans syndrome, Dwarfism, AMC
b. Acquired- Rheumatoid Arthritis , Stills disease
c. Others- Scheuermanns disease, Osteogeneis
imperfecta
D. Truamatic type-
a. Vertebral- fractures, Irradiations, Surgery
b. Extravertebral- Burns, Thoracogenic
E. Metabolic
F. Nutritional/ Endocrinal
G. Miscellaneous
7. Congenital Scoliosis Classification:
• According to the area of the spine affected
– Cervical, Cervico-thoracic,
– Thoracic
– Lumbar
– Lumbo -sacral spine
• According to the pattern of deformity
–Kyphoscoliosis,
– Lordoscoliosis
8. Classification
Given by Winters, Moe and Eilers
A. Failure of formation
1. Partial failure of formation (wedge vertebra)
2. Complete failure of formation (hemivertebra)
B. Failure of segmentation
1. Unilateral failure of segmentation (unilateral
unsegmented bar)
2. Bilateral failure of segmentation (block vertebra)
C. Miscellaneous
16. Causes
• Vertebral anomalies that result in imbalance
of the longitudinal growth of the spine
• Prevalence rate is 1/1000 live births
• Critical time for segmentation of vertebrae is
5th to 6th weeks of intrauterine life
• No genetic etiology has been found
17. Natural history
• Curve progression occurs more rapidly during first
five years of life and during adolescent growth
spurt.
• 6 monthly x-ray- to evaluate progression of curve
• Most severe- concave, unilateral unsegmented bar
with a convex hemivertebra –unilateral segmented
bar- double convex hemivertebra - block vertebra.
• Rate of severity- more in- Thoracolumbar then in
thoracic then upper thoracic region.
18.
19. Clinical evaluation
History-
• Chronologic age.
• Age at recognition of deformity
• Rate of progression of deformity.
• Associated symptoms- Pain, fatique, Cardiopulmonay
symptoms,
• Developmental factors.
• Rate of growth.
• Appearance of secondary sexual characteristics
• Menarchy
• Genetic factors- similar deformity in other siblings.
20. General physical and systemic
examinations
1. Cardiopulmonary system
• Pulmonary study- blood gas analysis, lung
volume, Breathing mechanics, Blood gas
distribution
• Cardiac study- ECHO, Marfans syndrome
2. Growth factors-
• Height- Compared with parents, other siblings
• Dentition
• Secondary sexual characteristics
21. 3. Evidence of underlying conditions
• Spinal dysraphism- pigmented hairy patch
• Neurofibromatosis- skin tumour , Cafe au lait
spots
• Club foot, calf atrophy, absent reflexes,
atrophy of one lower limb compared to other
22. Local examinations
1. Skin of back- hair patches, lipomas, dimples,
scars
2. Trunk alignment-
• Concave side- lower shoulder, prominent iliac
creast, chest less prominent
• Convex side- high shoulder, shift of thoracic
cage, head shifted towards concave side
23.
24.
25.
26. 4- Symmetry of shoulder girdle.
• neck shoulder angle
5. Assessment of specific curves.
6. Pelvic obliquity.
28. Radiological evaluation
1. Erect film- Anteroposterior, lateral, Oblique
Stagnara derotation view – cassette is placed
parallel to the medial aspect of rotational rib
prominence and x-ray beam is positioned to the
right angle of the cassette
2. Recumbent films
3. Right and lateral bending films- AP view
4. Spot lateral view of LS spine- to rule out
spondolisthesis
29.
30.
31.
32. • CT scan with 3-D reconstruction
• MRI
• Diagnosis by Sonogram
• Can be done before birth
• Can be done at birth or soon after
Clinical diagnosis
• Deformity
• Associated congenital problems.
36. Treatment
• Conservative methods
Cast or brace (Milwaukee)
• Indications
A- Flexible long curve
B- Skeletal immaturity
- Control compensatory curve.
- No evidence in affection the prognosis.
- Can be fitted to 2 years old child.
37. Posterior fusion without
instrumentation
• Ideally done for small curves which have
documented progression or predicted to progress
• Controversy Posterior vs Combined AP
Posterior alone can prevent progression but
drawback is crankshaft phenonmenon
38.
39.
40. Combined AP fusion
Combined is reserved for
•Sagittal plane problems
•To increase flexibility of the scoliosis by discectomy
•To eliminate anterior physis to prevent bending of torsion of the
fusion mass with further growth(Crankshaft)
•To treat curves with significant growth potential
41. Posterior fusion with instrumentation
• Done for large curves in older children where
casting/bracing would not obtain or maintain
the correction
• Used to increase the fusion rate and as a
stabilising strut, rather obtaining a significant
correction
• Goal is modest correction and curve control
42.
43.
44. Advantages of intrumentation
• Rate of pseudoarthrosis is less.
• Correction attained is slightly more
• No post operative discomfort of bracing
45. Risks/Disadvantages of instrumentation
• Use of rods in small children in whom the bone structure is not strong enough to add
any stability
• Excessive distraction leading to paralysis
• Failure to preoperatively evaluate for a tethered cord or other intraspinal
abnormalities
• Failure to do a wake-up test after rod insertion
• Failure to perform adequate fusion because of reliance on internal
stability
• Failure to supplement the instrumentation with adequate external immobilization
46. Combined AP convex
hemiepiphysiodesis and fusion
Indications:
1. Children <5 years
2. A documented progressive curve
3. A curve< 50 degrees
4. A curve of <6 segments
5. Concave growth potential
6. No pathological congenital kyphosis
or
lordosis
48. Combined AP hemiepiphysiodesis and fusion
• This technique has practically no role in case where there is
failure of formation
• This considered to the most advantageous for treating single
hemivertebra which has not resulted in large curves at the time of
surgery
• Post op cast immobilisation is needed for 6 months
50. Thoracic insufficiency sydrome
• Inability of the thorax to support the normal
respiration and lung growth
• Occurs in congenital scoliosis because of ribs fusion
on concave side
• Lung growth is limited by the anatomical boundaries
of the thorax
• Lung volume becomes 30% adult size whereas
thoracic spine becomes 2/3 of adult sitting height
51.
52. Vertical expandable prosthetic
titanium ribs
• A technique to directly treat the chest wall deformity
with indirect correction of congenital scoliosis
• This allows the treatment of total global deformity of the thorax,
allowing spine to grow undisturbed by surgical intervention