Case Review #14: 23 year old with Progressive Adult Idiopathic Scoliosis
•
2 likes•1,956 views

A 23 year old female presented with Progressive Idiopathic Scoliosis with extreme pain. She would require a posterior spinal fusion from T4 to L2.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Case Review #14: 23 year old with Progressive Adult Idiopathic Scoliosis
Similar to Case Review #14: 23 year old with Progressive Adult Idiopathic Scoliosis (20)
More from Robert Pashman
More from Robert Pashman (20)
Recently uploaded
Recently uploaded (20)
Case Review #14: 23 year old with Progressive Adult Idiopathic Scoliosis
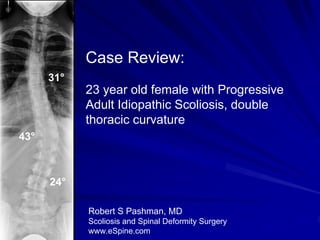
- 1. Case Review: 31° 23 year old female with Progressive Adult Idiopathic Scoliosis, double thoracic curvature 43° 24° Robert S Pashman, MD Scoliosis and Spinal Deformity Surgery www.eSpine.com
- 2. Patient History 23 year old female. Upper thoracic and thoracolumbar curve with a lumbosacral transitional vertebra. Patient also has spina bifida occulta distally in the lumbar spine. Thoracic curve 31°. Thoracolumbar curve progressed from 38° to 43°. Compensatory curve 24°. Patient was a ballerina at one time. Therefore, we will get a CT scan of her lower lumbar spine to rule out the possibility of her having a pars fracture at the transitional vertebra, which is distal. www.eSpine.com
- 3. Progressive Curvature The patient’s curvature progressed 5° over a six month period. 31° She has a significant thoracolumbar curve of 43°, with 38° 43° sharp angular apical segment at T11-T12. The patient has unremitting low back pain, 24° discomfort, imbalance in the frontal and sagittal plane, and wishes surgical stabilization. Sept, 2007 March, 2008 www.eSpine.com
- 4. Pre-op X-rays The patient has a 31° upper thoracic curve, a 43° thoracolumbar curve, and a 31° compensatory 24° curve. Her sagittal balance is negative, and she has 43° significant hyperlumbar lordosis. This is not the issue. 24° Due to the hyperlumbar lordosis, the patient’s Hyperlumbar head is not balanced over her body. lordosis www.eSpine.com
- 5. Bending X-rays On side bending to the right, her L thoracolumbar curve is significantly R flexible. She has a 6th lumbar vertebra with L5-S1, which is not well seated in the lumbar spine, and it is also noted on left side bending that the patient has significant flexibility of her lumbar curve with straightening of 2 to the left of the mid plum. www.eSpine.com
- 6. Bending X-rays L R www.eSpine.com
- 7. Indications for Surgery 1. Type III CN progressive 43° thoracolumbar Adult Idiopathic Scoliosis. 2. Progressive increasing low back pain. 3. Failed conservative therapy. 4. Significant rotation, with cosmetic deformity due to rib hump. 5. Spina bifida occulta and possible anatomic anomaly. www.eSpine.com
- 8. Surgical Strategy The strategy would be from T4 down to L2. The T4 level is because of the depression of the right shoulder and the structural nature of the proximal curve, and the L2 vertebra is because on side bending, the patient horizontalized L2 over the mid sacrum and L3 is neutrally rotated. Segmental spinal instrumentation using CD Legacy 1/4-inch 5.5 stainless steel rod-screw construct from T4-L2. This would be a 10- level instrumented fusion. Posterior spinal fusion, T4-L2, using locally harvested autogenous bone and RH BMP. Apical spinal osteotomy, Smith-Peterson radical osteotomy, T9-T10, T10-T11, T11-T12, T12-L1. Intralaminar decompression for lateral recess stenosis, T12-L1, L1- L2 bilaterally. Intraoperative SSEP motor evoked potential analysis. Intraoperative fluoro. www.eSpine.com
- 9. Post-Op Films Moderately flexible thoracolumbar curve. After the osteotomy, the curve was highly reducible. There was significant residual rotation at the distal L2. The patient is balanced in both the frontal and sagittal planes. Frontal plane Sagittal plane www.eSpine.com
- 10. Pre-Op/Post-op Comparison 31° The patient’s curve was corrected 43° 14° from 43° to 14°. She is balanced in the frontal plane, and her rib hump was reduced, and her 24° shoulders are now even. www.eSpine.com
- 11. Pre-Op/Post-op Comparison The patient’s hyperlumbar lordosis has been corrected, and her sagittal alignment has been restored. Her head is now directly over her body. www.eSpine.com