Downloaded 250 times















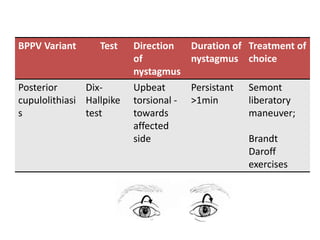
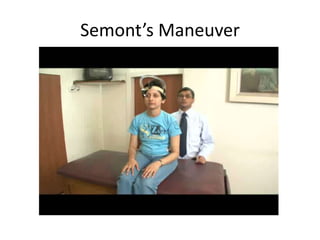


















Benign paroxysmal positional vertigo (BPPV) is a common inner ear condition characterized by brief episodes of vertigo triggered by changes in head position. It is caused by debris in the semicircular canals leading to abnormal signals in the vestibular system. BPPV involving the posterior semicircular canal accounts for about 94% of cases. Diagnosis is made through provocative positional tests like the Dix-Hallpike maneuver. Treatment involves repositioning maneuvers like Epley's maneuver to move the debris out of the affected canal. BPPV typically resolves spontaneously within weeks to months, but recurrence is possible in about 15-45% of cases within a year without treatment.










































































