1. Radiological identification of skeletal structures can determine if bones are present, if they are human, estimate age and sex, and detect abnormalities.
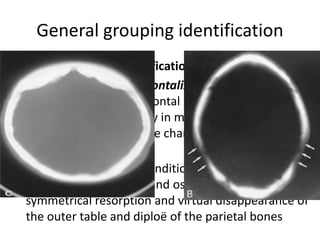
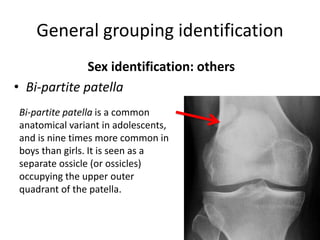
2. Sex can be estimated by examining pelvic traits like the subpubic angle and skull traits like parietal thinning.
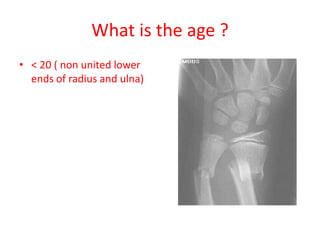
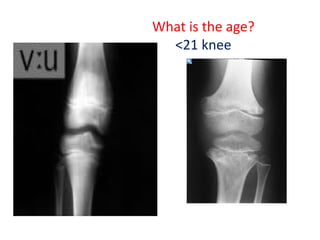
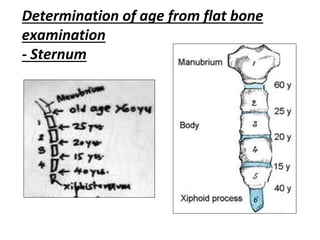
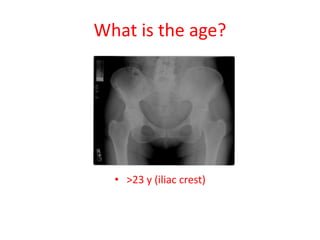
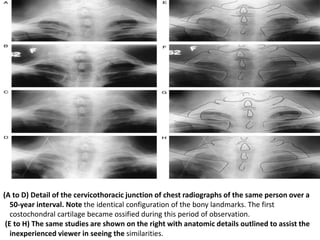
3. Age can be estimated by examining ossification of epiphyseal plates and their fusion, as well as degenerative changes to bones.
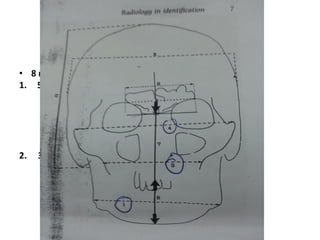
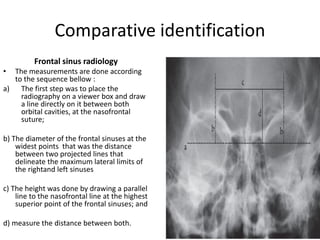
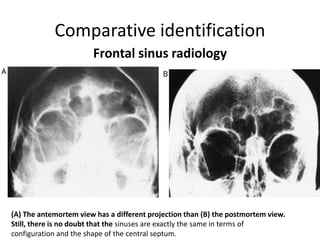
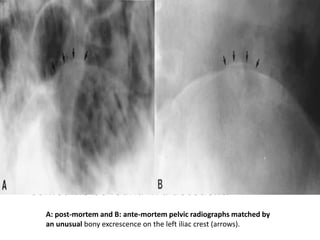
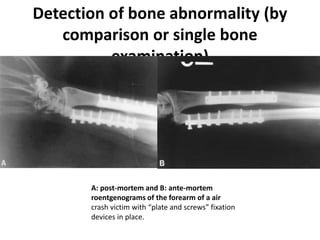
4. Comparative identification through radiological examination of traits like the frontal sinus patterns can help identify unknown remains.