Downloaded 2,639 times












![DIDN’T HEAL A = Another wound : Competition for the substrates required for wound healing. L = Low temperature : (relatively) distal aspects of the upper and lower extremities (a reduction of 1-1.5°C [2-3°F] from normal core body temperature) is responsible for slower healing of wounds at these sites.](https://image.slidesharecdn.com/woundcare-091130124157-phpapp02/75/Woundcare-15-2048.jpg)


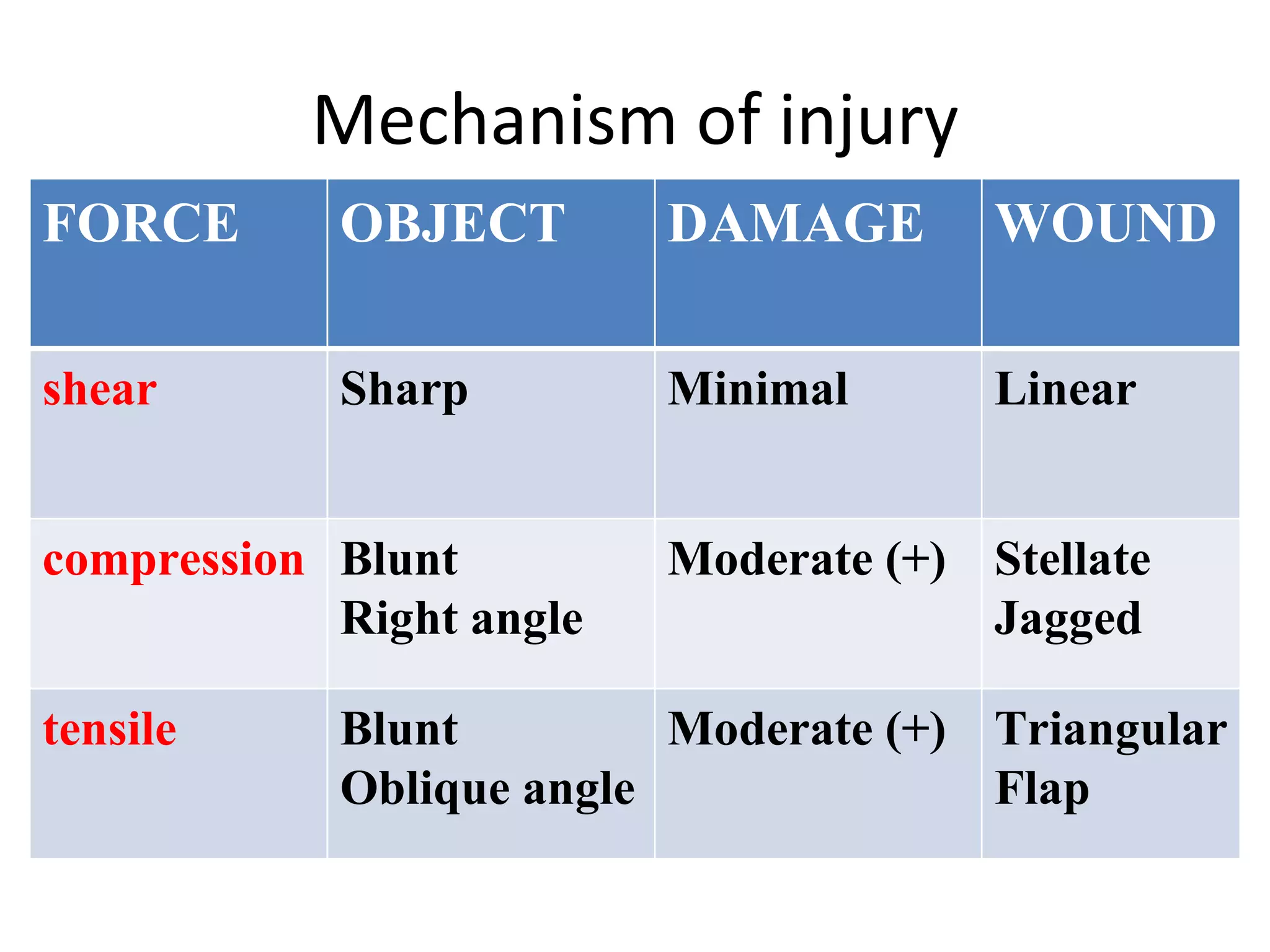

































The primary goal of wound care is facilitating the natural healing processes rather than technical repair alone. Wound healing involves inflammatory, proliferative, and remodeling phases. Wound preparation includes anesthesia, hemostasis, debridement, cleaning, and closure or dressing. Factors like infection, nutrition, tissue ischemia, and tension can impair healing. Proper wound evaluation and management are essential for optimal healing outcomes.