4. Definition ofport-a-Cath
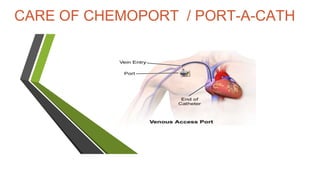
• Aport-a-Cath, is animplanted device which allows easyaccessto apatient’s
veins. A port-a-Cath is surgically-inserted completely under the skin and
consists of two parts –the portal and the catheter.
5. • It is made from asilicone bubble and appears asasmall bump under the skin.
• Theportal, made of special self-sealing silicone, can be punctured by a
needle repeatedly before the strength of the material is compromised.
• Its design contributes to avery low risk of infection.
8. Indication of port-a-Cath
Difficult cannulation
Long term access – can be used for many years
Central line for blood drawing and medication administration
May administer continuous infusion IV vesicants
Ports placed for patients receiving chemotherapy , generally restricted
to chemotherapy infusions only
Lowest incidence of catheter- related bloodborne infections
Low maintenance care at home
10. • PPE (personal protective equipment )
• Dressing tray/Trolley
• Huber needle with luer lock extension tubing
• Chlorhexidine 2%Gluconate with 70%IsopropylAlcohol solution
• 5ml, 10mLsyringe
• Normal saline
• Sterile dressing set (Gauze, Pad, Kidney tray)
• Transparent occlusivedressing
• Tape/ Tegaderm (8526 )
• Inj Heparin(1:10 ml ns / Inj hep lock (no dilution )
Articles / Equipment needed for procedure
11. PROCEDURE
• Position patient in low fowlers position.
• Expose IVAD site and palpate port.
• Assemble equipment and create sterile fields with the opened packages.
• Wash Hand, Mask and gloves.
• Cleanse port site with disinfectant in a circular motion from center of
port outward to cover an area approximately 4" in diameter.
• Repeat three times and allow to air dry 1 minute, and then wipe any
excess with sterile gauze.
12. • Attach saline filled syringe and prime the tubing and needle.
• Leave syringe attached to set and close the clamp.
• Be careful to maintain the sterility of the Huber needle
13. • Palpate the port system with the non-dominant hand and stabilize
the port edge with 2 or 3 fingers.
• With the dominant hand, using firm, consistent pressure, insert the
non-coring needle at a 90 degree angle) to the port septum until
the back of the port chamber is located.
• Rotate site with each access if last access site known.
• Open the clamp on the extension tubing and verify patency by
aspirating for blood return and instilling saline.
• Slowly flush the system with 10mL of saline, disconnect syringe and
close clamp.
14. • secure the needle and tubing to the Patient,
• using the 4-inch occlusive dressing.
15. • HEPARIN LOCKING
After saline flush, ports areflushed heparin to lock the system for intermittent access,
when discontinuing access,and every 4 weeks to maintain patency.
EQUIPMENT
• 10mLsyringecontaining5mLHeparinLock FlushSolution (100units/mL)
• 10mLsyringecontaining10mLsterile normal saline
• Chlorhexidine2%Gluconatewith 70%IsopropylAlcohol swab
PROCEDURE
1.Cleansetop of adaptor with Chlorhexidine2%Gluconatewith 70%IsopropylAlcohol
swab.Allow to dry completely.
2.Attach syringeto adaptor.
3.Openclampon extensiontubing.
4.Verify patency and inject saline,disconnectsyringe.
5. Inject heparinsolution.
6. Disconnectsyringeand clampextensiontubing.
16. IVTHERAPY
• EQUIPMENT
• 10mLsyringewith 10mLsterile normal saline
• tape
• intravenous solution asordered with primed tubing
• Surgiprep
• PROCEDURE
• 1.Cleanseadaptor withsurgiprep allow toair dry.
• 2.Attach salinefilled syringeandassessfor patency.
• 3.Connectprimed IVto 3 way extension
• 4.Cleanseconnectionsite with alcoholswab,allow to dry.
• 5.Secureconnectionwith waterproof tape.
• 6.Infuse asper physician’s order.
• Note: Whendiscontinuing anIVinfusion,flush the port with 10mLnormal saline then 1mL
• heparin solution(1000units)
18. PROCEDURE
• Apply sterilegloves.
• Prepare 10mlsnormal salinein 10-ml.syringe.
• Prepare 1mls heparin solution in 10mlsyringe. ( with dilution 10 ml NS)
• Cleanthe adaptor with asurgiprep
• Attach a10mLsyringe.
• Withdraw the required amount of blood by attaching a10ml syringe
• Flushthe IVADwith 10mLnormal saline
• NSflush/heparinflush
• resumeIVtherapy.
19. EQUIPMENT
PEE
5mLsof heparin lock flush solution in 10mLsyringe
10mLs sterile normal saline without preservative in 10mLsyringe
2" x 2"gauze
Bandaid
20. REMOVING AN IVAD NEEDLE (GRIPPER)
PROCEDURE
• If IVinfusing, stop IV.
• Applygloves.
• Cleanse injection port or adaptor with Chlorhexidine 2%Gluconatewith
70%IsopropylAlcohol solution and allow to air dry.
• Attach 10mLsyringe with 10ccnormal saline, aspirate for blood return
then instill saline
• Disconnect salinesyringe.
• Attach syringe with 1 mLsHeparin Lock FlushSolution and inject.
• Loosen dressing fromneedle site.
• Apply pressureto edges of port with 2 or 3fingers while withdrawing the
needle straight
Apply pressureto the port site with a2" x2" gauze until bleeding stops
and micropore / tegaderm
22. Complication.
after accessing
Occlusion issues if not accessed or flushed properly
Skin breakdown
Infection
Thrombus formation
Catheter fracture or migration
23. Patienteducation 1-afterportinsertion (post operative)
• Limit activity for 24 hour
• Sterile dressing for 24 hr. if no drainage present (changedressing daily or
if needed)
• Transparent dressing till wound healing
• Notify physician if any complication (pain, fever, swelling, other)
24. Patienteducation 2- during in patient using port
• Do not sleep on site of port
• Observethat line is not kinked
• Low activity when connected with pump
• Mal-position ofneedle
• Extravasation
• Notify physician if any complication (pain, fever, swallowing, other)