CVAD Management, Care and Maintenance (Radiology Nursing)
•Download as PPT, PDF•
7 likes•4,006 views

CVAD Management, Care and Maintenance (Radiology Nursing) June 2016

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (16)
Similar to CVAD Management, Care and Maintenance (Radiology Nursing)
Similar to CVAD Management, Care and Maintenance (Radiology Nursing) (20)
Recently uploaded
Recently uploaded (20)
CVAD Management, Care and Maintenance (Radiology Nursing)
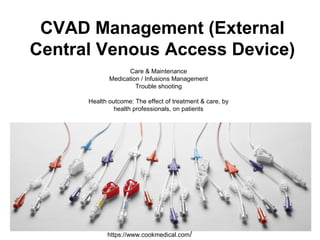
- 1. CVAD Management (External Central Venous Access Device) Care & Maintenance Medication / Infusions Management Trouble shooting Health outcome: The effect of treatment & care, by health professionals, on patients https://www.cookmedical.com/
- 2. What is a CVAD? Two main categories • External Devices - Percutaneous or non tunnelled CVADs Short term inserted into the subclavian, jugular or femoral veins - can remain insitu for maximum 7 to 10 days ie. Central Venous Catheter, Mid-line, • Internal Devices Long term PICCs (Peripherally Inserted Central Catheters - up to 6 to 12 months (can be classified as short term if insitu for less than 30 days Totally implantable CVAD – Ports - for up to 5 years Long term CVADs Hickman’s / apheresis Hickman’s/ permacaths, tunnelled CVAD’s with a Dacron Cuff etc. can remain insitu for years
- 3. Pressure Injectable vs. Non pressure injectable Pressure Injectable lines are central venous access devices. - Can tolerate 290 psi and not exceed 300 psi - For pressure injection of contrast media - Power injectable lines have a power injectable or psi rating
- 4. Infection Control Did you know? Preventing infection is the responsibility of all staff and can be achieved with the implementation of asepsis during the insertion, ongoing care and maintenance and final removal of the device. http://medind.nic.in/jat/t14/i2/jatt14i2p359.htm http://standinguptopots.org/treatment/iv
- 5. Catheter related blood stream infection occurs • At a rate of 23 per 1000 catheter days • Has an 11% mortality rate (392 deaths every year from a preventable adverse event Casey, A. L., L. A. Mermel, et al. (2008). "The Lancet Infectious Diseases." 8 (12): 763-776. Bolz et al(2008) Management of CVCs in ICUs in Australia Healthcare Infection 13:48-55 mededucation.org esicm.org
- 6. 5 Moments of Hand Hygiene THHS has adopted the World Health Organisation (WHO) 5 moments for Hand Hygiene. Healthcare workers should perform hand hygiene with an Alcohol-Based Hand Rub (ABHR) or an antimicrobial liquid soap solution: as defined in the THHS Hand Hygiene Procedure. Gojo.com hha.org.au
- 7. Risks vs. Benefit of CVAD • CVAD pose a greater risk to the patient when compared with Peripheral Intra-venous Cannula (PIVC). • They are most commonly used in a patient group that are more susceptible to complications; the critically ill, the immuno-suppressed, for haemodialysis and for long term therapy options. • These devices are vital in keeping the patient alive www.curamedical.grwww.telefelx.com
- 8. What are the nursing requirements? Medical Imaging staff are required to document their assessment in the patients’ record. - The type, side location and Insertion date of each CVAD recorded in ieMR - Ensure site checks every 12 hours - Observation of redness at/or surrounding the insertion site. Redness or erythema can indicate the presence of an exit site infection. - Inflammation or swelling at/or surrounding the insertion site. This may indicate extravasation, infiltration or infection - Pain at / or along the path of the vein, this may indicate phlebitis. -Has the patient had any fevers or rigors? This may indicate infection in the line. - When accessed does the CVAD bleed and flush easily? - Has the external length of the catheter increased/decreased? - Does the patients limb appear swollen or painful IF YES, STOP AND PROBE FURTHER ilearnexternal.health.qld.gov.au
- 9. Accessing and De-accessing of a CVAD Competency skill • Only staff who have successfully completed and been deemed competent using the relevant Skills Checklist are able to provide the relevant care for CVAD • This competency must be reassessed annually. • Final competency assessment of an individual staff member must be entered into the THHS Staff Education Database by the CNC/ NUM / NE / MO of their local work environment
- 10. Assessment & Detection of CVAD • The patient • Check the external catheter • Dressing • Bung • Flushing (Resistance) & Lock requirements • Infusional Regimes • X-Ray • Occlusions • Air embolisation • Infiltration & Extravasation • Tip Migration
- 11. Check the patient The insertion site should be visually inspected by the clinician hourly with continuous infusions and at least every 12 hours if no infusion, for erythema, drainage tenderness, swelling, suture integrity and catheter position. More frequent assessments are necessary when using high-risk solutions and medications. CVADs no longer clearly needed should be promptly removed. infuserveamerica.comwww.midwest-nursing.com
- 12. CVAD Dressings • Dressing type and replacement intervals • Dressing type Replacement interval • Transparent, semi-permeable, • self-adhesive polyurethane Weekly • Gauze Second daily • Chlorhexidine-impregnated Weekly • *All dressings should be replaced routinely as well as when the dressing becomes damp, loosened, no longer occlusive or adherent, soiled, if there is evidence of inflammation, or excessive accumulation of fluid. Manufacturer’s recommendations should be followed • Measurement of the external catheter should be documented on the CVAD management plan every shift (morning, evening & night).
- 13. CVAD bungs • What to use? • Negative Pressure • Neutral Pressure • Positive Pressure Positive displacement mechanical valves are designed to reduce retrograde flow into the catheter more effectively than standard luer connectors. Pulsatile flushing is used to create turbulence & clean inside of Catheter. If using positive displacement devices DO NOT clamp until syringe is removed from injection bung.
- 14. CVAD flush and lock requirements • Flushing the CVAD maintains patency, prevents the mixing of incompatible medications or solutions, and reduces the build-up of intra- and extra-catheter material such as fibrin or blood. CVADs should be flushed at established intervals if used intermittently. The flushing of central venous catheters is recommended: - before and after medication administration - administration of blood and blood products - intermittent therapy - after obtaining blood specimen - when converting from intermittent therapy - when the device is not in use *https://www.health.qld.gov.au/clinical-practice/guidelines-procedures/diseases-infection/infection-prevention/intravascular- device-management/default.asp
- 15. Flush technique Flush solution is 0.9% Normal Saline, the volume will need to be between 10-30mls – this will depend on the catheter, size and length. When flushing use a push-pause technique and a minimum of a 10ml syringe, this creates turbulence and assists in freeing the lumen of debris.
- 16. Medication/infusion management When a CVAD requires accessing for therapy, it is recommended to - have a continuous, closed circuit - maintain patency - reduce manipulation - reduce infective complications Infusions must be changed immediately on suspected contamination or when the integrity of the product or system is compromised. As per The Townsville Hospital Policy, all clinicians should not disconnect and reconnect an administration set (e.g. showering, toileting or threading through patients’ clothing, etc.).
- 17. Post Care of PICC • The anatomical placement of the catheter tip must be documented in the patient record and checked prior to the initiation of any therapy through the device. Following catheter insertion, a chest X- ray may be obtained to: • verify catheter placement • detect adverse events such as a pneumothorax • retain as a record of placement (Povoski, 2005). • Catheters may change position when the patient moves. PICC lines can move two centimetres away from the head with arm movement. www.radiologyassistant.nl radiopaedia.org
- 18. CVAD tip migration The causes of CVAD tip migration can include: - normal anatomical forces/bodily movements that increase intrathoracic pressure i.e. breathing, coughing, sneezing, vomiting or strenuous upper extremity movements such as golf or weight lifting. - forceful flushing. - Catheters can be damaged at several points along the catheter line both internally and externally. - At the catheter hub - Applying a cap before the cleansing solution has dried will effectively ‘glue on’ the cap which can result in cracking of the hub of the lumen. - Near the catheter hub or below the bifurcation. Use the correct clamps or smooth blade forceps to reduce the risk of damage to the catheter. - Above the catheter bifurcation damage to external catheter sections can be repaired, however this should be considered as a temporary measure until the catheter can be replaced. Repair increases the risk of infection, haemorrhage and air embolis. Only some PICCS, not all. - The catheter internally CVADs have the potential to fracture and if fragments are not detected and removed there is a risk of mortality, due to injury/perforation of the atria, ventricles, and myocardium, pericardial effusion, cardiac tamponade, cardiac arrhythmias and pulmonary embolism.
- 19. Occlusions There are two (2) main types of occlusions 1. Persistent withdrawal occlusion is when the catheter will flush but there is an inability to withdraw blood. This decreases the function of the catheter, but also reduces the ability to check the patency of the catheter 2. Total occlusion is where the practitioner cannot infuse fluids into the catheter or withdraw blood. Another potential complication of CVAD’s is DVT (Deep Vein Thrombosis).
- 20. Non-thrombotic occlusions • Mechanical obstructions are a common and can be due to external or internal factors. • External refers to those occlusions that are part of the CVAD that is external to the body. • Internal refers to occlusions that are part of the CVAD inside the body. • Chemical occlusions are the other type of non-thrombotic occlusion External - kinked Subclavian vein insertion with catheter pinched between clavicle and first rib Internal
- 21. Thrombotic occlusions Thrombotic occlusions may occur due to: - a fibrin sheath or tail forming on the catheter tip acting as a one- way valve permittant infusion, but not withdrawal of blood. - a mural thrombus when the fibrin from the catheter surface binds with fibrin from a vessel wall injury and forms a venous thrombus - fibrin deposits and/or sludge accumulation within a portal reservoir - an intra-luminal thrombosis/ blood clot
- 23. Air embolism • Air embolism occurs when intrathoracic pressure is less than atmospheric pressure, allowing air to enter the patient’s venous circulation through the open end of the catheter. • Cardiac output, venous return, and coronary artery flow are decreased. Vascular collapse, arrhythmias, hypoxemia, hypercapnia, neurological deficits and death may ensue. Air embolisim in the pulmonary truck
- 24. Infiltration and Extravasation • Infiltration is defined as the inadvertent administration of non-vesicant solutions or medications into tissues surrounding the catheter. • Extravasation is defined as the inadvertent administration of vesicant solutions or medications into tissues surrounding the catheter. Extravasation can lead to tissue necrosis, pain, infection, loss of mobility of the extremity and surgical procedures. Fatality following extravasation has been reported. Anthracycline (chemotherapy) Extravasation Area of skin necrosis after extravasation of intravenous fluid
- 25. Review of CVAD Management Let’s review… • Pre injection • Post injection • Documentation
- 26. The Quick facts – Pre-injection • Assessment and identification of the pressure injectable CVAD, insertion date, site etc. • Hand Hygiene • Aseptic Technique • Dressing pack • 70% chlorhexidine & 2% alcohol cleansing solution • 3 swabs, 15 seconds • Let the cleaning solution dry for 20-30 seconds • Unlock CVAD • Access the CVAD site with aseptic, non touch technique • Aspirate blood via the lumen, then pulsate flush with 0.9% Normal Saline. • 3 swabs, 15 seconds • Let the cleaning solution dry for 20-30 seconds • Connect with pressure injector • Assess pressure injection pressures when injecting
- 27. • Hand Hygiene • Aseptic Technique • Dressing pack • 70% chlorhexidine & 2% alcohol cleansing solution • 3 swabs, 15 seconds • Let the cleaning solution dry for 20-30 seconds • Access the CVAD site with aseptic, non touch technique • Access the lumen, then pulsate flush with 0.9% Normal Saline. • Disconnect syringe • Clamp CVAD device • Document in ieMR The Quick facts – Post injection
- 28. Documentation In ieMR we must document: • That you have used an aseptic technique to access the CVAD • whether the CVAD pre-injection aspirated and flushed without issues with 10ml Normal Saline 0.9% • whether the CVAD post-injection flushed without issues with 10ml Normal Saline 0.9% • Medication infusion administered
- 29. More information? Infection control regularly provides courses on CVAD management - CVAD skills checklist - CVAD procedures
- 30. Interesting case 1 Tama Galiere was only 10 months old when he died on 25 June 2008 at the Children’s Hospital in Randwick. He was receiving intravenous antibiotic treatment via a central line for a severe infection of his left eye. The tip of the PICC migrated into the ventricle. How can this have happened? Migration of PICC line into the heart ventricle seems to be quite common. Migration may occur as a result of stretching and flexing movements of the body but this will usually account for a migration of no more than 1.5 to 2 cms. Any migration of the tip beyond that will be limited by the length of line within the body and, in Tama’s case, will have been influenced by whether any redundant length of line was inserted into his body at the time of the installation of the line or subsequently. http://www.coroners.justice.nsw.gov.au/Documents/galiere%20findings%209%20%20may%2014%20%20final.pdf
- 31. Interesting case 2 Left-sided PICC (highlighted in yellow) with end tip abutting lateral wall of the SVC www.nursingcenter.com Interesting case 2 This PICC tip is against the wall of the SVC. This is a risk for extravastion.
- 32. Thank you!
Editor's Notes
- CVAD Management (External Central Venous Access Device) Care & Maintenance Medication / Infusions Management Trouble shooting Health outcome: The effect of treatment & care, by health professionals, on patients
- What is a CVAD?Two main categories External Devices - Percutaneous or non tunnelled CVADs Short term inserted into the subclavian, jugular or femoral veins - can remain insitu for maximum 7 to 10 days ie. Central Venous Catheter, Mid-line, Internal Devices Long term PICCs (Peripherally Inserted Central Catheters - up to 6 to 12 months (can be classified as short term if insitu for less than 30 days Totally implantable CVAD – Ports - for up to 5 years Long term CVADs Hickman’s / apheresis Hickman’s/ permacaths, tunnelled CVAD’s with a Dacron Cuff etc. can remain insitu for years
- Pressure Injectable vs. Non pressure injectable - Minimise long term intravenous access attempts on difficult or unwell patients for CT interventions - Check insertion documentation. Power PICCs can be identified by a pink and purple hub.
- Preventing infection is the responsibility of all staff and can be achieved with the implementation of asepsis
- Some interesting facts The cost in Australia is estimated to be between 25.7 million and $95.3 million each year.
- 5 Moments of Hand Hygiene Before touch a patient Before a procedure After body fluids exposure After touching a patient After touching a patients surroundings
- Every CVAD has the potential for complications such as infiltration, extravasation, exit site infections, phlebitis, occlusions including thrombus formations or blood stream infections. Appropriate management of the CVAD is crucial to prevent such complications. The following information will assist staff in providing optimal care and management of the CVAD.
- Nursing assessment of the CVAD insertion site is imperative for the prevention or early identification problems. It is the nurse’s responsibility to document this assessment and initiate care that will prevent complications.
- All Staff must meet the following competency criteria to practice Accessing & De-Accessing a CVAD within THHS. Training and education on the CVAD provided by specialty units where this procedure is common place, this includes but not limited to Oncology, Intensive and Neonatal care Units, Renal Unit, Medical Imaging etc. Successfully perform a directly supervised CVAD Access & De-Accessing competency skills checklist. The assessor must be currently competent in the procedure to perform the assessment
- You need to assess the CVAD and detect any issues prior to accessing it
- The CVAD catheter should be inspected for changes in line integrity (kinks, splits). Review of the CVAD should be documented in the patient record each shift. Patients should be encouraged by the clinician to report any discomfort such as pain, burning, swelling or bleeding. If pus is present at the insertion site, swab the site prior to cleaning and send for culture. If systemic symptoms are present blood cultures from a peripheral vessel/PICC and all lumens must be obtained (fever or other signs of sepsis), e.g. tachycardia, tachypnoea, hypotension.
- These are the types of dressings and the replacement intervals. If the dressing is damp or soiled etc. it should be replaced. The Measurement of the external catheter should be documented on the CVAD management plan every shift (morning, evening & night).
- The displacement action expels a small amount of the solution used to flush the catheter when the syringe used for flushing is disconnected from the luer. Pulsatile flushing is used to create turbulence & clean inside of Catheter. If using positive displacement devices DO NOT clamp until syringe is removed from injection bung.
- All intravenous access ports should be meticulously cleaned by the clinician with a single-use 70% alcohol-impregnated swab or 2% alcoholic chlorhexidine vigorously for a minimum of 15 seconds and allowed to dry prior to accessing the system*. For example a typical intermittent infusion of medication may involve swabbing the access port: - before the initial saline injection to assess catheter patency, - before attaching the sterile infusion tubing or syringe, and - before flushing and/or locking the catheter with saline after administering the medication.
- Syringes smaller than 10ml have been shown to exert excess pressures on the catheter. These may damage the catheter.
- Infusions must be changed immediately on suspected contamination or when the integrity of the product or system is compromised. Intravenous infusion bags, lines and burettes require frequent changing to prevent infection through the contamination of these devices. As per the national recommendations for user applied labelling these devices require labels to be applied. As per The Townsville Hospital Policy, all clinicians should not disconnect and reconnect an administration set (e.g. showering, toileting or threading through patients’ clothing, etc.). If disconnected from the patient, the fluid bag, burette and administration set must be discarded and a new fluid bag, burette and administration set reconnected.
- Catheters may change position when the patient moves. PICC lines can move two centimetres away from the head with arm movement; subclavian or jugular catheters can move two to three centimetres towards the head. The initial catheter tip position in the lower third of the superior vena cava may have a final position in the upper end of the superior vena cava .
- CVAD tips can spontaneously migrate at any time during an indwelling period. This is more common in long-term devices. Migration is usually into the internal jugular vein. It should never be assumed that the CVAD tip will not move after initial insertion. Any deviation of the CVAD tip from the lower SVC can lead to the development of; catheter dysfunction; catheter fracture/migration; venous thrombosis; venous perforation; cardiac tamponade.
- Resistance when flushing a CVAD may be the first signs of an impending CVAD occlusion. These occlusions include non-thrombotic and thrombotic causes. Another potential complication of CVAD’s is DVT (Deep Vein Thrombosis
- Mechanical obstructions are a common and can be due to external or internal factors. External refers to those occlusions that are part of the CVAD that is external to the body. Includes kinked or clamped IV tubing, Clamped CVAD lumen, or tight sutures around the insertion site. Internal refers to occlusions that are part of the CVAD inside the body. Includes CVAD tip malposition, catheter abutment against a valve or vessel wall, compression of the catheter itself by the clavicle and the first rib, known as pinch-off syndrome damage or malposition of catheter or needle. Chemical occlusions are the other type of non-thrombotic occlusion, caused by precipitates or lipid deposits from infusions of incompatible solutions.
- Thrombotic occlusions may occur due to a fibrin sheath or tail forming on the catheter tip a mural thrombus when the fibrin from the catheter surface binds with fibrin from a vessel wall injury and forms a venous thrombus fibrin deposits and/or sludge accumulation within a portal reservoir an intra-luminal thrombosis/ blood clot
- This is a few pictures of some intraluminal thombus
- Air embolism occurs when intrathoracic pressure is less than atmospheric pressure, allowing air to enter the patient’s venous circulation through the open end of the catheter. The bolus of air travels to the right ventricle impeding the blood outflow in the pulmonary artery. Cardiac output, venous return, and coronary artery flow are decreased. Vascular collapse, arrhythmias, hypoxemia, hypercapnia, neurological deficits and death may ensue. The degree of harm caused is directly related to the gauge of the CVAD insitu, the volume of air infused, the rate of air entry and the patient’s position at the time of the event.
- Infiltration is defined as the inadvertent administration of non-vesicant solutions or medications into tissues surrounding the catheter. Extravasation is defined as the inadvertent administration of vesicant solutions or medications into tissues surrounding the catheter
- Lets review Pre injection Post injection Documentation
- Assessment and identification of the pressure injectable CVAD, insertion date, site etc. Hand Hygiene Aseptic Technique Dressing pack 70% chlorhexidine & 2% alcohol cleansing solution 3 swabs, 15 seconds Let the cleaning solution dry for 20-30 seconds Unlock CVAD Access the CVAD site with aseptic, non touch technique Aspirate blood via the lumen, then pulsate flush with 0.9% Normal Saline. 3 swabs, 15 seconds Let the cleaning solution dry for 20-30 seconds Connect with pressure injector Assess pressure injection pressures when injecting
- Hand Hygiene Aseptic Technique Dressing pack 70% chlorhexidine & 2% alcohol cleansing solution 3 swabs, 15 seconds Let the cleaning solution dry for 20-30 seconds Access the CVAD site with aseptic, non touch technique Access the lumen, then pulsate flush with 0.9% Normal Saline. Disconnect syringe Clamp CVAD device Document in ieMR
- In ieMR we must document: That you have used an aseptic technique to access the CVAD whether the CVAD pre-injection aspirated and flushed without issues with 10ml Normal Saline 0.9% whether the CVAD post-injection flushed without issues with 10ml Normal Saline 0.9% Medication infusion administered
- Infection control regularly provides courses on CVAD management QHEPS onlineSharon CNC - CVAD skills checklist - CVAD procedures
- Tama Galiere was only 10 months old when he died on 25 June 2008 at the Children’s Hospital in Randwick. He was receiving intravenous antibiotic treatment via a central line for a severe infection of his left eye. The tip of the PICC migrated into the ventricle. Migration may occur as a result of stretching and flexing movements of the body but this will usually account for a migration of no more than 1.5 to 2 cms.
- This PICC tip is against the wall of the SVC. This is a risk for extravastion. Left-sided PICC (highlighted in yellow) with end tip abutting lateral wall of the SVC
- Thank you!