6. S G :Quantity &Function
Your salivary glands make
a quart of saliva each day
1000:1500 CC
It increase during meal
and decrease after 20 years age .
Saliva is important to:
- lubricate our mouth,
- Help with swallowing,
- Protect your teeth against bacteria,
agent.- produce antibacterial
- produce enzymes Aid in the
digestion of food.
21أيار2017 6Prof Basma Moussa
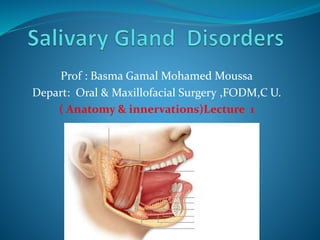
7. Classification of Salivary Glands
Major & Minor
salivary Glands
- Parotid glands
Present around
mandible & insides
the cheeks
- Submandibular
glands
at the floor of
the mouth
- Sublingual glands
under the tongue
- Minor gland
present all over
mouth & throat
21أيار2017 7Prof Basma Moussa
The three major
pairs of salivary
glands are
8. Major SG Minor SG
The major salivary glands are called
“major” because they are big,
-It has its own duct that leaves the
gland and opens into the mouth to
deposit saliva.
-There are 3 pair major salivary glands
on each side of the face and neck:
- They are called “minor” because
they are much smaller,
- have no envelope around them .
don’t have an organized outflow
system leading up to a duct..
-The minor salivary glands are found
all over the mouth and throat.-
21أيار2017 Prof Basma Moussa 8
9. Embryology
SG developed from
embryonic oral cavity
as buds of epithelium
extended to
underlying CT ,
- It start at 8 weeks IU-
21أيار2017 Prof Basma Moussa 9
10. Basic salivary Gland unit consisted
of :
S G unit consisted of :
myoepithelial cell -
21أيار2017 Prof Basma Moussa 10
11. SG embryology & Anatomy
Major SGMinor SG
Day 35at 40 dayIntra uterine I U
6 ( 3 pairs)1000-1500Number
Parotid
Submandibilar
Sublingual
1.Labial
2.Buccal
3.Palatine
4.Tonsiller
Weber ‘s gland
5 . Retomolar
6. Lingual
-Inferior apical ( glands
of Blandin an of Nuhn)
- Tast buds ( Ebner’s
glands)
- Posterior lubricating
glands
-
Types
21أيار2017 Prof Basma Moussa 11
12. The 3 major SG
21أيار2017 Prof Basma Moussa 12
13. Parotid gland
Superiorly – Zygomatic arch.
Inferiorly – Inferior border of the mandible.
Anteriorly – Masseter muscle.
Posteriorly – External ear and sternocleidomastoid.
21أيار2017 Prof Basma Moussa 13
14. Parotid gland
It is the largest salivary gland,
It have 2 loops superficial (big) & deep (small)
It sandwich the mandible in front of ear.
The parotid gland tapers down at the bottom into what is
called the “tail” of the gland.
Its duct, called Stenson’s duct, 6cm length & 1:3 mm
diameter. May also accessory duct with accessory gland .
21أيار2017 Prof Basma Moussa 14
15. Parotid gland
It is the only salivary gland to have lymph nodes within
its envelope..
The facial nerve extends into the middle of the parotid
gland where it fans out into five branches to muscles
of facial expression. And divide it to deep &
superficial lobes.
21أيار2017 Prof Basma Moussa 15
16. Submandibular Salivary G Sublingual Salivary Glands
The two submandibular glands are in the
submandibular triangle, below the jawbone.
The ducts Wharton’s ducts, open just under
the tongue in the floor of the mouth.
Each duct is about five centimeters long. 2:4
mm diameter.
The marginal mandibular branch of facial
nerve, moves the lower lip downwards on each
side.
Other nerves in close association with this
gland include the hypoglossal nerve (which
moves the tongue) and the lingual nerve
(which supplies sensation and taste to the
tongue and mouth region).
Under the tongue in the floor of
They meet in the midline.
The ducts are called ducts of Rivinus
( 8-20)they open directly into the mouth.
Some of these ducts even unite and form the
major ducts of Bartholin, which meet
submandibular duct.
The lingual nerve is the main nerve to
consider. It runs along the side of the gland
until it gets to the front, and then it goes
underneath the gland, where it runs with the
submandibular duct until it goes up into the
tongue.
21أيار2017 Prof Basma Moussa 16
17. Minor S G’
You have about thousand of
minor salivary glands all over the
mouth and throat.
They are most concentrated in a
few places, including the
junction of the hard palate with
The soft palate,
In the lips
The inner lining of cheeks.
On the tongue and even down into
the throat.
21أيار2017 17Prof Basma Moussa
18. For any question
My e- mail is : basmagm@yahoo.com
Cell no : 01005644098
21أيار2017 Prof Basma Moussa 18
23. Composition of normal saliva
The electrolyte
composition of
saliva higher
concentrated in
parotid than
submandibular
gland except
calcium twice than
parotid .
Viscosity of saliva
more in sublingual
gland then
submandibular
then parotid .
21أيار2017 Prof Basma Moussa 23
25. innervations
The control of saliva derived from stimulation of:
Parasympathatic N
It have
preganglioic
nerve to ganglia
to post ganglionic
nerve to gland
from superior
cervical ganglion to
the glands via the
arterial blood
supply
Sympathetic N
21أيار2017 Prof Basma Moussa 25
26. Innervations of SG
Postganglio
nic Cranial
Nerve
sensory
supply
parathympath
-atic
Ganglia
Parasympathati
c N via Ganglia
Sympathat ic
N via arterial
plexus
Gland
Via auriculo-
temopral
nerve V 3
Otic GGlossopharyng N
no 9
To
lesser petrosal n
Inferior cervical
ganglion via plexus
on external carotid
artery
Parotid
Lingual N
V3
Submandibular
G
Facial N to
chorda
tympani N
(facial nerve)
Superior salivatory
Nucleus via arterial
plexus of the face
Submandibular
Gland
Lingual N
V3
Submandibular
G
Facial N to
chorda
tympani N
(facial nerve)
Superior salivatory
Nucleus via arterial
plexus of the face
Sublingual-
gland
21أيار2017 Prof Basma Moussa 26
30. History & clinical examination
Most important
component of
diagnosis:
- Patient will
guide the doctor
like :
1. events that
occurred with
complain.
2. back history
or recurrent
symptoms .
3. sometimes this
information let dr to do or
ignore to make any further
diagnostic evaluation
21أيار2017 Prof Basma Moussa 30
31. End of clinical exam by
categorization of the lesion
- Developmental
- Reactive
-- Obestructive
-- Inflamatory
-- Infectious
-- Metabolic
-- Traumatic
-- Neoplastic
--
21أيار2017 Prof Basma Moussa 31
36. •
Swelling in right parotid
Long standing painless
Swelling.
Q: is there any need for
more diagnostic
modalities?
•21أيار2017 •Prof Basma Moussa •36
37. Swelling in lower lip
Few days
History of trauma
Red bluish in color
Slight discomfort
21أيار2017 Prof Basma Moussa 37
53. Stone in parotid duct &
submandibular
21أيار2017 Prof Basma Moussa 53
54. Submandibular stone
% Rate
10% in parotid
80 % in submandibular gland
5% sublingual gland
N B
15- 20 % of all stone not appear in radiograph except if
stone completely calcified
21أيار2017 Prof Basma Moussa 54
55. Sialography
21أيار2017 Prof Basma Moussa 55
Amount :
0.5 to 1 ml
Injection of
radioopaque
material inside
SG
Duct.
Types
-Water soluble
material
- Oil- based
70. U S oncoytoma of submandibular gland
21أيار2017 Prof Basma Moussa 70
71. Salivary scintigraphy.
This nuclear medicine test involves the intravenous
injection of a radioactive isotope, which is tracked over
the course of an hour to see how quickly it arrives in all
your salivary glands.
21أيار2017 Prof Basma Moussa 71
80. Sialogram
endoscopy
-It is a small video
camera (endoscope)
With light at end of
flexible cannula )
- It is diagnostic or
therapeutic
- it may use to dilate
small strictures .
-- Small metal baskets
used to retrieve stone
in ductal system
21أيار2017 Prof Basma Moussa 80
85. FNA
Biopsy
- using 20 gauge needle
To aspirate the cells.
-Immediate put in glass
slide and fixed for
histological
examination is it:
-ve ( Benign Tumor)
+ve( Malignant Tumor)
21أيار2017 Prof Basma Moussa 85
86. Biopsy
Uses of
Excision biopsy:
In minor salivary gland pathosis
As guide for major S G disorder
as in case of Sjogren’s syndrome
About 10 Minor SG (specimen
includes about 50
lymphocytes, histiocytes and
plasma cells per 4 mm cells
21أيار2017 Prof Basma Moussa 86
87. Sialo chemistry
Many electrolyte in saliva like Na, K, urea,
uric acid , glucose amino acids….etc,
If Na and K that means there is
sialadenitis.
fig. 1 Suction cup. The inner chamber is
placed over the duct orifice.
fig. 2 Application and simultaneous
collection on both sides is required.
fig. 3 Suction equipment.
21أيار2017 Prof Basma Moussa 87
88. Obstructive S G diseases
Sialolithiasis
Mucous retention & mucocele
Ranula
21أيار2017 Prof Basma Moussa 88
89. SG stone - Parotid stone
S& S:
-pain & swelling at meal.time
Check saliva flow from the
duct.
Check tenderness of the gland
Palpate the stone in floor of the
mouth.
Make radiograph. Hyperdense
lesion
21أيار2017 Prof Basma Moussa 89
91. Salivary stone surgical removal
Treatment :
-Anterior stone :
-Attempt to stimulate salivary flow to push the stone
-NB avoid to push the stone posterior
-Milk the gland to push the stone
-Posterior stone
refer to OMF surgeon may remove
The gland if there is continuous pain & infection
21أيار2017 Prof Basma Moussa 91
98. Quiz 1
What is anatomical structure found superior to the
parotid gland?
1. Inferior border of the mandible
2. Masseter muscle
3. Zygomatic arch
4. Sternocleidomastoid
:Submit Answer
21أيار2017 Prof Basma Moussa 98
99. Quiz 2
Questions
Where are the salivary glands in the mouth?
What glands are located under your chin?
What is the parotid gland?
What is sialadenitis of submandibular gland?
21أيار2017 Prof Basma Moussa 99
100. Quiz 3
* A Clinical evaluation of long standing parotid swelling
and it found that there is still continuous mild pain:
&Q: Is there any need for more diagnostic modalities?
why?
21أيار2017 Prof Basma Moussa 100
105. S & S of Acute bacterial sialadenitis
1. Rapid onset of periauricular swelling with pain &
erythema.
2. Purulent discharge from duct orifice.
3. Signs of inflammation.
Treatment:
1. I V Antibiotics,& culture & sensitivity test.
2. Analgesics.
3.I V fluid hydration.
4. I& Din some cases to prevent
Spread of infection that lead to
respiratory obstruction.
21أيار2017 Prof Basma Moussa 105
106. Mumps ?
S & S :
Fever ,
malaise ,
truisms,
in ability to eat ,
young age
21أيار2017 Prof Basma Moussa 106
107. Answer: mumps is a Viral non
suppurative infection
- Clinical feature :
-It is acute, contagious disease ,
- Incubation period 2:3 weeks.
- Epidemic in winter,
- It affect Parotid glands > submandibular >sublingualSG.
S & S
1. Painful,non erythmatous swelling of one or both
parotid glands ,
2- 6:8 year age,
3. Fever,cchills headach.
4.Resolve: 5:12 days , antipyretic, analgesics.
21أيار2017 Prof Basma Moussa 107
108. complication
1.Bacterial sialadinitis of the affected gland
2. Inflammation in gonads
3. Inflammation in CNS resulting in meningitis,
encephalitis ,
Orchitis ,
Deafness,
Myocarditis.
21أيار2017 Prof Basma Moussa 108
109. Treatment
Hydration : adequate I V fluids
Analgesics
Antipyretics
__________________________________________
If there are any superimpose bacterial infection
____________________________________________
-Antibiotics : Initial IV empirical A B like cephalosporin
( First generation) or Penicillin.
:Then: culture and sensitivity test of
purulent material
-:
21أيار2017 Prof Basma Moussa 109
110. 2.Necrotizing sialometaplasia
Definition :It is a reactive non-neoplastic inflammatory
process that involve palatal minor S G
Clinical age 23:66 year
Size : 1:4 cm
Mostly unilateral
Painfull deep ulceration.
21أيار2017 Prof Basma Moussa 110
111. 21أيار2017 Prof Basma Moussa 111
Unclear origin but maybe due to vascular infarction
of SG lobules
112. important
consideration
It is clinically &
histopathology
resemble SCC or MEC
-Histopath :for distinguish it
from malignancy >
-It may heal 6:10 weeks
spontinously
- No surgical ttt
-
21أيار2017 Prof Basma Moussa 112
113. histopathology is a part from Diagnosis :
it is nondysplatic appearances
21أيار2017 Prof Basma Moussa 113
114. Sjogren’s syndrome ( sicca )syndrome
It is autoimmune system
It is classified:
.11.Primary affect dry
mouth xerostomia and (
keratoconjuncti dry eye
2.Secondary : primary+ CT
disorder e g rheumatoid
arthritis,
-sex: female 9 > 1 male
- Age: 50 years age
21أيار2017 Prof Basma Moussa 114
122. Traumatic SG injuries
It may involve the duct, gland & facial nerve due to :
1. Fracture
2. Sharp Trauma
3.Car accident .
21أيار2017 Prof Basma Moussa 122
123. Management :
:Aspirate hematoma:
If Facial N anterior to vertical
line from lateral canthus of
no ttt:the eye to mental n
Surgical repair of Stenson’s duct
& facial nerve.
21أيار2017 Prof Basma Moussa 123
126. Neoplasm's
-incidence:
-1. SG tumors in major glands 80:85% > minor gland
15:20%
2. In Parotid more than submandibular & submental &
minor gland.
3. May be ulcer in malignant lesion or swelling
21أيار2017 Prof Basma Moussa 126
127. pleomorphic adenoma MRI
21أيار2017
Prof Basma Moussa 127
Mixed tumor , most common
Mean age45y
Male to female 3:2.
More in parotid & palate
Pleo :means many form.
Encapsulated
5% malignant
transformation
137. 1.Mucoepidermoid carcinoma
Most common malignant SG tumor :mucoepidermoid
carcinoma
10% major gland mostly parotid
20% minor gland mostly palate
Age :Above 45y
Sex: M to F ratio 3:2
Clinicl S&S: pain swelling or ulcer
Radiograph: & in intra bony may appear multilocular
posterior mandible :
21أيار2017 Prof Basma Moussa 137
138. Malignant pleomorphic adenoma
Second most common I O salivary gland malignancy
Site: palate, parotid
Sex: M to F ratio: 3-1 %
Age : 56y
S&S: Mostly asymptomatic & may ulcerated
Ttt: wide surgical excision
Prognosis : high recurrence rate
21أيار2017 Prof Basma Moussa 138
141. Grades ME C
There are 3 cell type;
1. mucous cells
2. Epidermoid cells
3. Intermediate cells
The higher the grade the more predominance of
epidermoid cells and pleomorphism.
21أيار2017 Prof Basma Moussa 141
142. Low grad adenocarcinoma
2ed most common Intra oral malignancy
Present between hard and soft palate.
(perinural invaion) Invade surrounding nerves
Treatment :
Wide surgical excision
Recurrence rate: 14%
21أيار2017 Prof Basma Moussa 142
143. ACC
3ed most common lesion:
Age : 53 y
Sex: m to f 3:2-
Site: 50% in parotid
Slow growing non ulcerated
Chronic dull pain
Perinural invasion leading to facial paralysis or in palate
lead to brain mass.
Ttt: wide surgical excision + radiation therapy
Prognosis: poor.
21أيار2017 Prof Basma Moussa 143
145. Treatment
IT NEEDS MULTIDISCIPLINARY TEAM: cancr care team
An evaluation should be done by individual head-and-neck specialists before
any treatment begins.
The team may include these specialists:
Medical oncologist: a doctor who specializes in treating cancer with
medication
Radiation oncologist: a doctor who specializes in giving radiation therapy to
treat cancer
Surgical oncologist: a doctor who specializes in treating cancer using surgery
Maxillofacial prosthodontist: a specialist who performs restorative surgery
in the head and neck areas
Otolaryngologist: a doctor who specializes in the ear, nose, and throat
Oncologic dentist or oral oncologist: dentists experienced in caring for
people with head and neck cancer
Physical therapist
Speech pathologist
Psychologist and/or psychiatrist
21أيار2017 Prof Basma Moussa 145
146. Also include:
Cancer care teams also include a variety of other :
-health care professionals, including “
1-physician assistants,
2-oncology nurses,
3-social workers,
4-pharmacists,
21أيار2017 Prof Basma Moussa 146
147. Treatment decision depends on
several Factors including:
1-The type, stage, and location of cancer
2- Possible side effects
3- The patient’s preferences and overall health
21أيار2017 Prof Basma Moussa 147
148. 1- Surgery
The goal of surgery is to remove as much of the tumor as
possible and leave negative margins.
. The type of surgery depends on the location and extent of
the tumor.
Types of surgery used to treat salivary gland cancer include:
1- Parotidectomy ( total or superficial )
If cancer has spread to the facial nerve, frequently a nerve
graft is necessary for the person to regain use of some facial
muscles.
21أيار2017 Prof Basma Moussa 148
149. 2-Endoscopic surgery. Occasionally, it is possible to
remove the tumor by endoscopic surgery (see
Endoscopy, under Diagnosis), which is less destructive
to healthy tissues than regular surgery. This is used
particularly when a salivary gland tumor begins in the
paranasal area (around the nose) or in the larynx. Or
during endoscopic surgery for what is believed to be
chronic sinusitis (inflammation).
3-Neck dissection. A neck dissection is when the
surgeon examines all of the critical structures in the
neck and removes lymph nodes from the neck. This
may be performed if the doctor suspects that the
cancer has spread.
21أيار2017 Prof Basma Moussa 149
150. 4-Reconstructive surgery.
Reconstructive (plastic) surgery may be used to replace
tissue and nerves that were removed during surgery to
eliminate the cancer.
-A prosthodontist is a dentist who specializes in
replacing teeth and parts of the jaw. Learn more about
cancer rehabilitation.
5- composit treatment that maen surgery followed by
radiation
21أيار2017 Prof Basma Moussa 150
152. 2- radiation therapy (used alone or
combined)
Radiation therapy is the use of high-energy x-rays or
other particles to destroy cancer cells.
A doctor who specializes in giving radiation therapy to
treat cancer is called a radiation oncologist.
A radiation therapy regimen (schedule) usually
consists of a specific number of treatments given over
a set period of time.
There are 2 main types of radiation therapy used for
salivary gland cancer:
21أيار2017 Prof Basma Moussa 152
153. A- External-beam radiation therapy. This is the most common type
of radiation treatment and is given from a machine outside the body.
External-beam radiation therapy may be used when a tumor has grown
into the soft tissue, has spread to the lymph nodes, or surrounds a
nerve.
Used in poorly differentiated tumors. (See the Stages and Grades
section for more information.)
A specific method of external radiation therapy, known as intensity
modulated radiation therapy (IMRT), allows more effective doses of
radiation therapy to be delivered while reducing damage to nearby
healthy cells.
Another type of external-beam radiation therapy used for salivary
gland tumors is proton therapy. At high energy, protons can destroy
cancer cells. Proton therapy may be used when a tumor is located close
to structures of the central nervous system, such as the brain and spinal
cord.
Internal radiation therapy. When radiation is given using implants,
it is called internal radiation therapy or brachytherapy. Internal
radiation therapy involves surgically implanting tiny pellets or rods
containing radioactive materials in or near the tumor.
21أيار2017 Prof Basma Moussa 153
154. Team work before radiation
. Radiation therapy can cause tooth decay. Often, tooth
decay can be prevented with proper treatment from a
dentist before beginning treatment. Learn more about
dental and oral health.
Other side effects from radiation therapy to the head and
neck may include redness or skin irritation in the treated
area, dry mouth (xerostomia)
or thickened saliva from damage to salivary glands, bone
pain, nausea, fatigue, mouth sores, and/or sore throat.
People may also experience pain or difficulty swallowing;
loss of appetite, often due to a change in sense of taste;
hearing loss, due to the buildup of fluid in the middle ear;
and buildup of earwax that dries out because of the
radiation therapy’s effect on the ear canal.
21أيار2017 Prof Basma Moussa 154
155. 3-Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells,
usually by stopping the cancer cells’ ability to grow and
divide.
Chemotherapy is given by a medical oncologist, a doctor
who specializes in treating cancer with medication.
. Common ways to give chemotherapy include an
intravenous (IV) or capsule that is swallowed (orally).
. A patient may receive 1 drug at a time or a combination of
different drugs at the same time.
Chemotherapy is not often used to treat salivary gland
cancer. Combining chemotherapy with radiation therapy
chemotherapy is most often used to treat later-stage cancer
or to relieve symptoms. Some chemotherapy drugs are
available in clinical trials that may treat cancer at an earlier
stage.
drugs can cause specific side effects
21أيار2017 Prof Basma Moussa 155
156. 4. Getting care for symptoms and side effects
- palliative or supportive care, treatment of side effects of
treatment and it includes :
supporting the patient with his or her physical,
emotional, and social needs.
-Palliative care is any treatment that focuses on reducing
symptoms, improving quality of life, and supporting
patients and their families
Nutritional changes, relaxation, emotional support
paliativecare-
21أيار2017 Prof Basma Moussa 156