
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Salivary gland.pptx
Similar to Salivary gland.pptx (20)
Recently uploaded
Recently uploaded (20)
Salivary gland.pptx
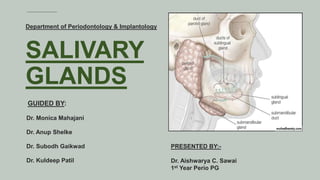
- 1. SALIVARY GLANDS GUIDED BY: Dr. Monica Mahajani Dr. Anup Shelke Dr. Subodh Gaikwad Dr. Kuldeep Patil PRESENTED BY:- Dr. Aishwarya C. Sawai 1st Year Perio PG Department of Periodontology & Implantology
- 2. CONTENTS: 1. Introduction 2. Classification of Salivary Glands 3. Development & Anatomy of Salivary Gland 4. Saliva 5. Clinical Significance and Applied Aspects 6. Reference 2
- 3. 01. Introduction Salivary glands are a group of organs secreting a watery substance that is of utmost importance for several physiological functions – a) protection of teeth and b) surrounding soft tissues c) lubrication of the oral cavity d) crucial for speech and e) perception of food taste. Salivary glands are exocrine glands that produce saliva. 3
- 4. 02. Classification of Salivary Gland Salivary glands can be classified based on their size, secretion, and function.
- 5. In human beings, three pairs of major salivary glands, are located outside the oral cavity, 1. Parotid gland 2. Submandibular gland 3. Sublingual gland 5 Numerous smaller minor salivary glands are located in various parts of the oral cavity. 1. Labial and buccal (mixed) 2. Glossopalatine (pure mucous) 3. Palatine (pure mucous) 4. Lingual (mixed) Size
- 6. 6 Secretion Serous – Watery secretion that contains enzymes such as amylase that aid in the digestion of carbohydrates. Mucous – Thick, viscous secretion that contains mucin, which lubricates and protects the oral cavity. Mixed – Contain both serous and mucous cells and produce a mixed secretion.
- 7. 7 Function Exocrine Glands - These glands secrete their products into ducts that empty into the oral cavity. Endocrine Glands - These glands secrete their products directly into the bloodstream and have a hormonal function.
- 9. (Para= around) , (Otic= ear) Largest Major Salivary gland. Paired organ. Purely serous gland. Weight= approx15 g. Resembles three-sided Pyramind. contributes approx 50% of saliva in the oral cavity. 9 1. Parotid Gland
- 10. Development of Parotid Gland:- The parotid gland is the first salivary gland to appear. Which starts developing in the 6th week of gestation via a process of proliferation, budding length, and branching. The parotid gland is ectodermal in origin near angle of stomedeum. The excretory ducts and acini derive from the ectoderm, whereas the gland's capsule and connective tissue come from the mesenchyme. Lau, C., & McGurk, M. (2019). Embryology of the Salivary Glands. Clinical Embryology, 165–168.
- 11. 11 The parotid gland appears behind the angle of the mouth, which is lined with buccal epithelium. This groove then closes to form the parotid duct which extends backwards. The distal end branches repeatedly and canalizes to form the acini of the gland. The duct recedes from the angle of the mouth to open in the vestibule of the mouth opposite the upper second molar tooth. The intimate relationship with the facial nerve is established from the beginning. Lau, C., & McGurk, M. (2019). Embryology of the Salivary Glands. Clinical Embryology, 165–168.
- 12. 12 6th gestational week – development begins 10th gestational week – arborization and canalization begins 18th gestational week – early secretions 28th gestational week – the maturation of the acini and ducts.
- 13. 13 Boundaries: The Parotid gland is bounded by the Superiorly- Zygomatic arch Inferiorly - External acoustic meatus Posteriorly- Sternocleidomastoid muscle Anteriorly- Masseter muscle External acoustic meatus
- 14. 14 Capsule of Parotid Gland Investing layer of the deep cervical fascia forms a capsule. It is supplied by great auricular nerve. The fascia splits to enclose the gland. The superficial lamina- thick and adherent to the gland, is attached to the zygomatic arch. The deep lamina -thin and is attached to the styloid process. A portion of the deep lamina, extending between the styloid process and the mandible, is thickened to form the stylomandibular ligament. Which separates the parotid gland from the submandibular salivary gland.
- 15. External Features:- Three borders:- 1) Anterior 2) Posterior 3) Medial Four surfaces:-1) Superior (base of pyramind) 2) Superficial 3) Anteriomedial 4) Posteriomedial
- 16. 16
- 17. 1. ARTERIES:- a) External carotid artery- enters the gland through its posteromedial surface. b) Superficial temporal artery c) Maxillary artery- leaves the gland through its anteromedial surface. d) Transverse facial artery- emerges at the anterior part of the superior surface. e) Posterior auricular artery- arise within the gland Structures within the Parotid Gland:-
- 19. 19 Superficial temporal artery Transverse facial artery
- 20. 20 Maxillary artery Posterior auricular artery
- 21. 21 2. Veins:- Retromandibular vein = Superfacial temporal + Maxillary vein
- 22. 9/1/2023 22 Anterior and posterior divisions of retromandibular vein The vein divides into anterior and posterior divisions. The anterior branch joins the facial vein form the common facial vein, where it drains into the internal jugular vein. Posterior branch joins the posterior auricular vein just below the apex of the parotid gland, forming the external jugular vein. Drains to:- Internal and external jugular vein. Drainage area:- Jaw, lateral skull, parotid gland, masseter muscle.
- 23. 23 Anterior division of retromandibular vein Posterior division of retromandibular vein
- 24. 24 Facial nerve:- Facial nerve courses through the parotid gland, without supplying any structure in it. origin :- The facial nerve (CN VII) arises from two divisions: a motor root and a smaller sensory root. Enters the gland through the upper part of its posteromedial surface.
- 25. 25 Course of facial nerve Intracranial course Intratemporal course Extracranial course
- 26. 26 Intracranial course motor fibres- motor nucleus of facial nerve superior salivatory nucleus (parasympathetic fibers) sensory fibres - nucleus of solitary tract (lower part of pons)
- 27. 27 Intratemporal course Branches greater petrosal nerve nerve to stapedius muscle chorda tympani
- 28. 28 Extracranial course As it exit from the stylomastoid foramen:- Posterior auricular nerve Digastric Stylohyoid
- 29. Terminal branches of Facial nerve Temporofacial Temporal Zygomatic Cervicofacial Buccal Marginal Cervical
- 30. 30
- 31. 31 • The gland is composed of a large superficial and a small deep part, the two being connected by an 'isthmus' around which facial nerve divides. Patey's faciovenous plane
- 32. Blood supply:- The parotid gland is supplied by the external carotid artery and its branches that arise within the gland. The veins drain into the external jugular vein and internal jugular vein.
- 34. 34 Inferior salivary nucleus IX nerve Tympanic nerve Tympanic plexus Lesser petrosal nerve Relay in otic ganglion Auriculotemp oral nerve Parotid gland Parasympathetic fibers
- 35. 35 Glossopharyngeal nerve Inferior salivatory nucleus Tympanic nerve
- 36. 36 Lesser petrosal nerve Tympanic plexus
- 37. 37 Otic ganglion Parotid branch of auriculotemporal nerve
- 38. From the lateral horn of T1 spinal segment preganglionic neuron arise. They ascends up and synapse in superior cervical ganglion. Postganglionic fibers pass through the otic ganglion and supply the parotid gland. Sympathetic fibers Sensory fibers Reach the parotid gland through the branch of mandibular nerve.
- 39. 39 Lymphatic drainage:- Only salivary gland with two nodal layers. Which drain into the superficial and deep cervical lymph system. They drain a. Temple b. Side of the scalp c. Lateral surface of the auricle d. External acoustic meatus e. Middle ear f. Parotid gland g. Upper part of the cheek h. Parts of the eyelids and orbit.
- 40. Parotid duct, also known as Stensen's duct. Roughly 7 cm x 3 mm long and leaves the superior part of the of the gland. It passes horizontally over the surface of the masseter muscle then courses medially toward the anterior border of the muscle. The duct then makes an abrupt right turn to cross the buccinator muscle and associated buccal fat pad, before opening into the buccal mucosa opposite the upper second molar tooth. Duct:-
- 41. 41 Accessory parotid :- It is salivary tissue present in close association or anterior to the Stensen's duct, lying on the masseter muscle but away from the main parotid gland. It exists in 21–61% of individuals Having blood supply from the transverse facial artery. Have secondary duct empting into the Stensen's duct. There are two types of anterior extension of the parotid gland: “facial process” which is attached directly to the main gland. “detached glandular mass” or “accessory parotid gland” which is completely separated from the main gland. average distance- 6mm. RamacharSM, HuliyappaHA.Accessoryparotidglandtumors.Ann MaxillofacSurg.2012Jan;2(1):90-3. doi:10.4103/2231-0746.95334.PMID:23483721;PMCID:PMC3591091.
- 42. Second largest. Paired major salivary gland. The gland is about the size of a walnut. It is roughly J-shaped. Mixed gland (mostly serous). Secretion by its duct against gravity into oral cavity. Lies in the submandibular fossa. Approx 70% of the saliva is produce in the unstimulated state. 2. Submandibular gland
- 43. 43 Location located within the submandibular (digastric) triangle of the neck.
- 44. 44 -The submandibular gland develops after the parotid gland in the later part sixth week. -The gland originates from endodermal buds. -These epithelial buds develop into solid cords, which canalize to form the submandibular ducts. Development of Submandibular gland:-
- 45. 45 Development begins with the appearance of a groove between the tongue and the gums, the alveololingual groove. This groove then closes to form the submandibular duct. The distal end of the duct then grows backwards along the floor of the mouth, branches repeatedly and canalizes to form the acini of the gland. The anterior end of the duct proceeds forwards to open adjacent to the frenulum of the tongue. The striated and intercalated ducts develop by 16 weeks, and the acinar cells predominate by 24 weeks.
- 47. 47 Boundaries of superficial part a. Inferior surface. b. Lateral surface. c. Medial surface.
- 48. 48 Relations of deep part Present in between mylohyoid and hyoglossus Laterally - Mylohyoid Medially - Hyoglossus Above - Lingual nerve with submandibular ganglion Below - Hypoglossal nerve
- 49. 49 It is supplied indirectly by the external carotid artery through the branches of the facial and lingual arteries. Relation of facial artery:- The facial artery is related to the superficial part of the gland twice. At first, it grooves the posterior end of the gland. Then it descends on the lateral surface of the gland to reach the base of mandible at anerio-inferior angle of masseter. Venous drainage follows a similar pattern. BloodSupply
- 50. 50 • Lymph passes to submandibular lymph nodes. • The lymph nodes associated with the submandibular gland are not within the gland’s capsule but instead are located adjacently in the submandibular triangle. • The submandibular lymphatics comprise 3 to 6 nodes, beneath the body of the mandible. • The nodes are palpable on the superficial surface of the submandibular gland. Lymphatic Drainage
- 51. Submandibular Duct:- Main excretory duct is the Wharton duct. This duct, approx. 5 cm in length and 1.5mm in diameter. It starts from the medial surface of superficial part of gland near the posterior border of mylohyoid. Ducts makes a loop (genu) around the posterior border of mylohyoid inside the gland. Then emerges from deep part. It runs forward and slightly upward.
- 52. 52 3. Sublingual gland Smallest salivary glands. Paired exocrine glands. Almond shaped. Weighs about 3 to 4 g. Considered a mixed serous and mucous gland. Predominantly a mucous gland. Contributes approx 5% of saliva in the oral cavity. Produces a thick mucinous fluid and lubricates.
- 53. The sublingual gland first appears in the eighth week of prenatal development. The sublingual gland arises as a small bud developing from the alveololingual groove. These buds attain a common sheath and appear as one gland having several openings into the floor of the mouth. These epithelial buds develop into cords, which canalize to form the sublingual ducts and also form the mucous acini. Development of Sublingual gland:- Lau, C., & McGurk, M. (2019). Embryology of the Salivary Glands. Clinical Embryology, 165–168.
- 54. 54 Relations Front - Meet with opposite side gland Behind -Comes in contact with deeper part of submandibular gland Superiorly- by the tongue Below - Mylohyoid muscle Lateral - Sublingual fossa Medial -Genioglossus muscles
- 55. 55 Sublingual artery The sublingual glands receive their primary blood supply from the 1) Sublingual artery - branches of the lingual artery. 2) Submental artery- branches of the facial artery. These arteries are both branches of the external carotid artery. Submental artery BloodSupply
- 56. 56 Sublingual vein The sublingual vein drains into the lingual vein, which then flows into the internal jugular system.
- 57. Nerve supply (Submandibular Ganglion) It is a Parasympathetic ganglion. It is a relay station for secretomotor fibers supplying submandibular and sublingual glands. It is topographically connected to lingual nerve ( branch of trigeminal nerve). It is functionally related to chorda tympani (branch of facial nerve). Location -lies on the hyoglossus muscle just above the deep part of the submandibular salivary gland, suspended from the lingual nerve by two roots. Relations :- Above- lingual nerve Below – deep part of submandibular gland Medial – hypoglossus muscle Lateral – superficial part of submandibular gland
- 58. 58 It has three roots:- PARASYMPATHETIC: is derived from facial nerve (chorda tympani). SYMPATHETIC: is fromT1 spinal segment. SENSORY: is from lingual nerve. Roots of submandibular ganglion
- 59. 59
- 60. 60 Branches to submandibular gland: 5-6 branches from the ganglion conveying postganlionic parasympathetic, sympathetic and sensory fibers to the submandibular gland. Branches to sublingual gland: these reach the sublingual gland via the lingual nerve through the anterior root of submandibular ganglion. Branches
- 61. Major sublingual duct of Bartholin. Minor sublingual ducts of Rivinius. About 15 ducts emerge from the gland Open along sublingual folds Excretory duct
- 62. 04 Saliva Saliva is the principle protector of the soft & hard tissues. Saliva is a clear, watery fluid that is produced by the salivary glands. It plays a crucial role in the digestive process and oral health. Saliva is composed of water, electrolytes, enzymes, and antibacterial compounds. When the process of secretion diminishes, the oral tissues become susceptible to infection and the ability to masticate, swallow, speak & taste may be disturbed. 62
- 63. 63 Properties of saliva:- 1)Volume:- Total saliva secretions :- > major salivary glands - 90%. a) submandibular gland – 70% b) parotid gland – 25% c) sublingual gland – 5% > minor salivary glands - 10%.
- 64. 64 The normal daily production of saliva varies between 0.5 and 1.5 liters. Resting (unstimulated) state - approx two-thirds by submandibular glands. Upon stimulation - 50% by parotid glands. Unstimulated saliva flow rate is approx 0.3-0.4 ml / min. During sleep - decreases to 0.1 ml / min. During eating, chewing and other stimulating activities - increases to about 0.4-0.5 ml / min. 2) Reaction :- Saliva has a pH normal range of 6.2-7.6 with 6.7 being the average pH. Resting pH of mouth does not fall below 6.3. (Baliga S, MuglikarS, Kale R. Salivary pH: A diagnosticbiomarker. J IndianSoc Periodontol.2013 Jul;17(4):461-5) 3)Tonocity:- saliva is hypotonic to plasma. (IorgulescuG. Saliva betweennormal and pathological.Importantfactorsin determining systemicand oralhealth.J MedLife.2009Jul-Sep;2(3):303-7.)
- 66. 66 Salivary components Components & their concentration / function Electrolytes Sodium– 2-21mmol/L Potassium– 10-36 mmol/L Calcium– 1.2-2.8 mmol/L Magnesium– 0,08-0.5 mmol/L Chloride– 5-40 mmol/L Bicarbonate25 mmol/L Phosphate– 1.4-39mmol/L Major salivary proteins Alpha-Amylase. Acidic proline- rich proteins. Basic proline- rich proteins. Glycosylatedproline- rich proteins. Carbonic anhydraseVI. Histatins. Lactoferrin. Lysozyme. Mucins. Statherins. Galactosidase. Peroxidase,SuperoxideDismutase, Lactatedehydrogenase. dehydrogenase. Alkalinephosphatase. Maxtrixmetalloproteinase. Immunoglobulins. Salivary steroid hormones Cortisol,Testosterone,DHEA-s, Progesterone,Estradiol,Aldosterone. Aldosterone.
- 67. 67 Vila T, Rizk AM, SultanAS, Jabra-RizkMA. The powerof saliva: Antimicrobialand beyond. PLoSPathog.2019Nov 14;15(11):e1008058.
- 68. 68 Duct system 1. Intercalated ducts: smallest ducts, lined by cuboidal / flattened cells and open into Straited ducts. 2. Straited ducts: Lined by columnar cells and open into excretory ducts. 3. Excretory ducts: Lined by simple columnar epithelium
- 69. Two stages hypothesis of Saliva formation involves :- Stage I- Fluid secretion Stage II- NaCl Reabsorption & K Secretion. 69 Formation of saliva:- Catalán MA,NakamotoT, MelvinJE. Thesalivary glandfluidsecretionmechanism.J Med Invest. 2009;56Suppl:192-6.
- 70. Stage I- Fluid secretion
- 71. Stage II- NaCl Reabsorption & K Secretion
- 72. 72 Parasympathetic stimulation produces abundant quantities of watery saliva, Whereas sympathetic stimulation produces more viscous saliva (Bardow, Nauntofte and Pedersen, 2004).
- 73. 73 Salivary secretion is enhanced by two different types of salivary reflexes:- 1. Simple or unconditioned reflex. 2.Acquired or conditioned reflex.
- 74. 74 Simple or unconditioned reflex:- Food in mouth stimulate Chemoreceptors & pressure receptors initiate impulses in afferent nerve fibres impulses via extrinsic autonomic nerves salivary glands salivation
- 75. 75 Acquired or conditioned reflex:- >Salivation occurs without oral stimulation. >Just thinking about smelling, or hearing the preparation of pleasant food initiate salivation through this reflex. >a/c mouth watering.
- 76. 76 Salivary gland secretion Serous : very thin and and watery • Content: • -Amylase protein • -polysaccharides • -Cell:SerousCells Mucous: very thick and and viscous • Content: • -Mucins (glycoproteins) • -Carbohydrates • Cell: MucousCells Cells • Glands that secrete secrete this type: • 1. Palatine glands • 2. Posterior lingual lingual glands • All minor salivary gland exceptVon ebner’s gland. Mixed secretions: mix of of the two • Sublingual glands – – mostly mucous with with some serous. • Submandibular glands- mostly serous serous with some mucous • Anterior lingual glands.
- 77. 77 concentration substance Increases Protein, amylase, sodium bicarbonate. bicarbonate. Decreases Phosphate, urea, amino acid, uric acid, acid, serum, albumin Does not change Fluoride VARIATIONOFTHECONCENTRATIONOFCONSTITUENTSOF SALIVA WITHTHE INCREASE IN FLOW RATE
- 78. 78 Evaluation of salivary gland function Plays an important role in maintaining oral health. Should be included in the first visit of each new patient. There are standard questions that can identify patients with a high risk of salivary gland hypofunction. The four most common questions are: 1. Is the saliva flow rate too reduced, exaggerated or you can’t discern a difference? 2. Do you have difficulty swallowing? 3. Do you experience a dry mouth sensation during your meals? 4. Do you sip liquids to help with the swallowing of solid food? Iorgulescu G. Saliva betweennormaland pathological.Importantfactorsin determiningsystemicand oral health.J MedLife. 2009Jul-Sep;2(3):303-7.
- 79. 1. Avoiding foods with high sugar or acid, or high caffeine content, immediately before 2.Consumption of alcohol, nicotine within the prior 12 hours. 3.Vigorous physical activity and the presence of oral diseases or injury. 4.Not eating a major meal within 60 minutes of sample collection. 5.Rinsing mouth with water to remove food residue and waiting at least 10 minutes after dilution before collecting saliva. 6.Participants should not brush their teeth within 45 minutes prior to sample collection. 7.Dental work should not be performed within 24 hours prior to sample collection. 79 Saliva collection protocol
- 80. Wainwright in 1934 invent a method for saliva collection for the analysis of salivary calcium (Ca2+). In this method, the patient’s head was tipped forward with the mouth pointing vertically downwards and saliva was allowed to drip from the mouth into a filter funnel. 80 Method of saliva collection
- 81. Two pioneers companies(1990s) from the United States, namely Epitope, Inc. (now OraSure Technologies,USA) and Saliva Diagnostic Systems, Inc. (USA), developed commercially viable saliva collection devices. The OraSure Device was the first saliva collection device to be linked to a clinical test for the human immunodeficiency virus (HIV) and the company was successful in gaining Food and Drug Administration (FDA) approval for the device. 81
- 82. Other devices that have been used historically include the Salivette device and the Salimetrics Oral Swab (SOS). 82
- 83. 83 Whole saliva collection method Resting saliva Stimulated saliva 1. Draining method 2. Spitting method 3. Suction method 4. Swab method 1. Masticatory method 2. Gustatory method
- 84. Shannon et al. reported higher flow rate values in the standing position and lower values in the lying position as compared with the flow rate in the sitting position. Thus, it is ideal to collect saliva, while the subject is sitting upright with the head slightly tilted forward and the eyes open. The subject is made to sit quietly with the head bent down and the mouth open to allow the saliva to drip passively from the lower lip into the sterile tubes. Saliva collected by draining is without any stimulation and is more reliable. Draining method
- 85. Saliva is allowed to accumulate in the floor of the mouth and the subject spits out it into the preweighed test tubes. The advantage - it can be used when the flow rate is very low and where evaporation of saliva has to be minimized. The disadvantage - it might have some stimulatory effect, and hence cannot be used for unstimulated saliva collection. Spitting method
- 86. Saliva is allowed to accumulate in the floor of the mouth and aspirated continuously using micropipettes, syringes, saliva ejector or an aspirator. Suction method
- 87. It is performed by introducing a synthetic, pre-weighed swab or gauze sponge or cotton pad into the mouth, at the orifices of major salivary glands. The subjects are asked to chew(1-2 min) such that the sponge gets soaked within the saliva. Saliva soaked sponge is removed and placed in a sterile test tubes. Saliva is obtained by the saturated cotton using a needleless syringe or better by centrifugation. Though this method is less reliable & induce variations in saliva. To avoid this non-cotton based sampling are available: 1. Polystyrene foam swabs. 2. Rayon balls, such asOrapette (Trinity Biotech, Dublin, Ireland). 3. PolyesterSalivette (Sarsted, Newton, NC) Swabbing method
- 88. 88 Stimulated saliva may also be obtained using non absorbing methods: 1. Chewing a piece of paraffin wax of standardized size. 2.Chewing neutral gum base. 3.Chewing parafilm or rubber bands. 4. Keeping in mouth powdered drink crystals or other foodstuff containing citric acid.
- 89. It is strongly advised that only one type of collection device be used throughout. It is also recommended not to use the swab or suction method to collect unstimulated whole saliva because the swabbing action provides some degree of stimulation and thus increases variability. Samples obtained by spitting contain more bacteria than those obtained by drooling, which can affect further analysis of saliva compounds. Large volumes of saliva can be collected in a short time using the passive drooling method. 89
- 90. 90 GlandSpecific /GlandularSaliva I) Parotid saliva: The parotid duct open opposite to the upper second molars. Unstimulated parotid salivary flow is very low ; hence it is collected under stimulation. Citric acid solution (2-4% weight/ volume) is used for stimulation. Parotid saliva is collected using :- 1) Cannula or Lashley cup or ModifiedCarlsonCrittenden device. 2) Personalized plastic cups 3) Snail collector.
- 91. 91 ModifiedCarlsonCrittenden device The device has an outer and inner chamber. The inner chamber is attached to a plastic tubing. The outer chamber is attached to a rubber bulb or a suction device via plastic tubing and the cup is placed over the ductal opening. The suction device used may be dental suction unit, oil-free portable vaccum pump or laboratory suction bulb. It is found that an average of 1-1.5 ml of parotid saliva can be collected in 10-15 minutes. The disadvantages of this procedure are that it is complex, slow and invasive. It requires skilled expertise.
- 92. 92 II)Submandibular/ sublingual saliva This glandular saliva can be collected by 1. Cannulation 2. Segregator methods 3. Suction methods. 4. Wolfe apparatus
- 93. 93 Suction method: It is collected by blocking the Stensen’s duct using cotton roll or Lashley cup.Then, the saliva which gets accumulated in the floor of the mouth is aspirated using a syringe or micropipette or with gentle suction. Cannulation: Tapered polyethylene tubing can be used for cannulation of theWharton’s duct.The thin duct which is prone to rupture to be the biggest disadvantage of this method.
- 94. 94 Segregator method: An apparatus capable of collecting submandibular and sublingual saliva . The col-lector is placed on the lower jaw and the polyethylene tube connects the chamber to the collecting tube. The appliance should possess adequate peripheral sealing and proper retention to minimise the intermixing of submandibular and sublingual saliva and further eliminate the contamination by parotid saliva. The central chamber collects the sub- mandibular saliva, while the two lateral chambers collect sub-lingual saliva. The procedure is time consuming because the device has to be fabricated and adjusted on an individual.
- 95. 95 III)Collection of saliva from minor glands Saliva from minor salivary glands includes palatine saliva, buccal and labial saliva. Labial and buccal saliva can be collected using the periopaper / sialopaper absorbent method. The quantity of saliva can be determined by periotron. Palatine saliva is collected using filter paper (periopaper) or pipette method or by a collecting prosthesis.
- 96. Orageneis the most sophisticated technique, where preservatives are added to protect the sample integrity. All-in-one system for the collection, stabilization and transportation of DNA from saliva. New innovations in saliva collection
- 97. Oracol is based on saliva collection through an absorbent foam swab, which picks up 1 mL of saliva which is secure within the container. A micro tube is incorporated within the device, so that the saliva is centrifuged directly. This reduces the risk of aerosol contamination. This is particularly beneficial when used in the field, where laboratory facilities are not available.
- 98. 98 Saliva Collection Device manufactured by Oasis Diagnostics® Corporation; (A) Super•SAL™ and (B) Versi•SAL®. In contrast to cotton based collection methods that are reported to cause interference with certain biomarkers in saliva. More consistent sample uniformity. The sample obtained from either of these devices is a neat sample, meaning that there are no buffers required to dilute the specimen.
- 99. 99 A selection of different saliva collection devices used in medical and dental research. (A) Salivette® (Sarstedt); (B) Quantisal ® (Immunalysis); (C) SCS® (Greiner-BioOne).
- 100. 100 CHILDSALIVACOLLECTION METHODSAND DEVICES Due to the potential for choking when collection devices are placed in the mouth, collecting saliva from infants and children under the age of six requires special considerations. TheSalivaBioChildren’sSwab (SCS), for children under the age of 6 years, and TheSalivaBio Infant’sSwab (SIS), for infants under 6 months of age.
- 101. Specimens can be stored at room temperature (max 30-90 min). Thomadaki K et al., suggest that lowering the incubation temperature lowers the degradation rate of salivary proteome. Thus, immediately after saliva collection, it is recommended to freeze the samples at or below -20 ºC. If a freezer is not available, specimens can be stored at 4 ºC to prevent bacterial growth and further degradation of salivary molecules (no longer than 6 h) . Specimens can also be stored at -80 ºC for several years with little or no degradation. For RNA analysis, RNase inhibitor should be added in the supernatant fractions (not to pellet) before storing at -80 ºC. 101 Sample storage
- 102. 102 Snap-freezing of saliva in liquid nitrogen: Mix each saliva aliquots with an equal volume of 80% glycerol in H2O, then dip the sample in liquid nitrogen. This storage procedure aims to inhibit the bacterial protease activity degrading some salivary protein compounds, such as s-IgA.
- 103. The possibility of sampling error is highest during saliva collection and processing. Food and drinks should be restricted during saliva collection. food can be eaten up to 30 min (Granger DA et al) to 1 h before spitting (Beltzer EK et al). The individual should rinse his/her mouth with deionized water and wait at least 10 min before providing a specimen. Clear and comprehensible labeling is necessary for proper sample identification and handling. Permanent markers or bar-coded labels are highly recommended for long-term storage. 103 Sampling error & managment
- 104. Before collection, the optimal sample collection technique should be carefully chosen. Participants should be instructed precisely regarding the optimal placement and duration of the device or swab in order to ensure measurement accuracy. The collected saliva should be free of contamination. Sample contamination can be prevented by wearing gloves and using clean collection materials. After collection, the specimen should be stored appropriately. 104
- 105. Does psychological stress make a change in salivary protein secretion? It induce salivary alpha-amylase and cortisol levels. Salivary amylase level was observed to react more rapidly than cortisol during psychological stress, which could be a better indicator of stress. (Takai N et al) However, stress during dental treatment showed significant changes in the salivary cortisol and IgA levels than alpha-amylase (Ohura K et al) The concentration of IgA was found to be significantly elevated during the premenstrual or menstrual phase when compared with the postmenstrual phase.(Watanabe K et al) Based on above reports, we can anticipate that the salivary flow and secretory proteins can get varied in the healthy individuals. So, during saliva collection, we need to confirm from healthy volunteers that they are free from these kinds of psychological stress, which directly affect the saliva volume or salivary proteins.
- 106. 9/1/2023 106 Saliva as a diagnostic tool for periodontal disease: current state and future directions
- 107. Saliva act as a mirror of oral and systemic health.(kim et al. 2013) It is a valuable source for clinically relevant information. Because it contains biomarkers specific for the unique physiological aspects of periodontal ⁄ peri-implant disease. And qualitative changes in the composition of these biomarkers could have diagnostic value. By identifying patients with enhanced disease susceptibility, identifying sites with active disease, predicting sites that will have active disease in the future and ⁄ or monitoring the effectiveness of therapy. Introduction:-
- 108. 108 Salivaomics: Biomarkers and molecular signatures For generations, blood has medium of choice for diagnosis. But in recent years it has become evedient that salivary constituents can be detectable in diseased state. Introduced in 2008, the term "Salivaomics" aimed to highlight the rapid development of knowledge about various "omics" constituents of saliva, including 1. proteome(proteins), 2. transcriptome(messenger RNAs), 3. metabolome(metabolic compound), and 4. microbiome(microbes). salivaomics represents a novel approach in oral disease diagnosis, prognosis, and monitoring.
- 109. Advantages of salivary testing for diagnosis. Non-invasive, easy to use, inexpensive Safer to administer than serum sampling (no needles) Real-time diagnostic values No need for trained medical staff Multiple samples can be obtained easily Collection and screening can be done at home Minimal risks of cross-contamination More economical sampling, shipping and storage compared to serum Requires less manipulation during diagnostic procedures compared to serum Commercial availability of screening assays
- 110. 110 Limitations :- Salivary composition of biomarkers can be influences by method of collection and degree of stimulation of salivary flow. Changes in salivary flow rate may affect the concentration of salivary markers and also their availability due to changes in salivary pH Changes in salivary flow rate may affect the concentration of salivary markers. Many serum markers can increase in saliva in an unpredictable way for example oral wound.
- 111. The term "markers of disease" basically consists of three separate categories; (1) indicators of current disease activity; (2) predictors of future disease progression; (3) predictors of initiation of future disease at a currently healthy site The biomarkers provide “signature” of the health state
- 112. 112 NancySrivastavaet al., Pointof Care-A Novel Approachto Periodontal DiagnosisJournal of Clinical and DiagnosticResearch.2017Aug,Vol-11(8)
- 113. 113 LPS are triggered by gram-negative bacteria. PMNs as a first line defense Monocytes & macrophages respond to endotoxin. MMPs produced by fibroblasts & PMNs. TNF-a, IL-1b & receptor activator of of NF-kB ligand (RANKL) ICTP transported by byGCF or saliva GiannobileWV, BeiklerT, Kinney JS, RamseierCA, MorelliT, WongDT. Saliva as a diagnostictoolfor periodontal disease:currentstateand futuredirections.Periodontol2000.2009;50:52-64.
- 114. 114 Major salivary gland secretion mediators associated with periodontal diseases GiannobileWV, BeiklerT, Kinney JS, RamseierCA, MorelliT, WongDT. Saliva as a diagnostictoolfor periodontal disease:current stateand futuredirections. Periodontol2000. 2009;50:52-64.
- 115. 115 Antioxidants in saliva:- During inflammatory process Various ROS including oxygen-derived free radicles are produced, such as Superoxide (O), hydroxyl ion (OH), nitric oxide, hydrogen peroxide, and hypochlorous acid (HOCL). Antioxidant in saliva neutralized ROS such as Superoxide dismutase, glutathione peroxidase, peroxidase, catalase, etc. Antioxidant is defined as those substances which when present a low concentrations compared to those of an oxidizable substrate will significantly delay or inhibit oxidation of that substrate. (Battino et al. 2002, Zukowski et al. 2018)
- 116. 116 Markers of cellular damage and inflammation are 1. Lactate dehydrogrnase(LDH) 2.Aspartat aminotransferase(AST) 3.Alkaline phosphatase(ALP) 4.Alanine aminotransferase found in patients with rapidly progressive progressive periodontitis.
- 117. 117 Cytokines in saliva:- Ruhl et al (2004) estimated level of interleukin(IL)-1 alpha, IL-6, IL-8, epidermal growth factor(EGF), nerve growth factor(NGF), and albumin in parotid, submandibular, sublingual saliva. Various investigation have been done on correlation between salivary cytokines and periodontal status. Studies found elevated levels of IL-1beta in periodontitis patients.
- 118. 118 C- reactive protein (CRP) CRP levels are indicative of systemic inflammatory status. According toGiannobile et al (2009) there is relationship of elevated salivary & serumCRP levels in aggressive periodontitis. According toAzar et al (2011) study showsCRP level in saliva of smokers is increased than in non-smokers. GiannobileWV, BeiklerT, Kinney JS, RamseierCA, MorelliT, WongDT. Saliva as a diagnostictoolfor periodontal disease:current stateand futuredirections. Periodontol2000. 2009;50:52-64.
- 119. The concentration of LF:- • Unstimulated saliva- 8.96mg/L • Stimulated saliva- 7.11mg/L It is an important component of innate immunity. Salivary LF levels reduce after surgical periodontal treatment in chronic periodontitis patient. LF levels tend to decrease in smokers. Lactoferrin (LF)
- 120. IgA produced by the plasma cells of salivary glands. Two classes of IgA:- • IgA1- predominant in serum • LgA2- higher concentration in external secretions such as tears, saliva etc. They provide immunity towards various oral bacteria. 120 Immunoglobulins
- 121. 121 Lysozyme:- This enzyme has antimicrobial properties. It causes cleavage of chemical bonds in the bacterial cell wall, resulting in disruption of bacterial cell wall. Works on bothGram positive andGram-negative microorganisms. It has been reported that the patients with low level of salivary lysozyme are more susceptible to plaque accumulation.
- 122. Antimicrobial proteins in saliva. Primarily secreted by parotid and submandibular glands. Function is to neutralization of the endotoxic lipopolysaccharides located in membrane of Gram-negative bacteria. In human saliva atleast 12 histatins like peptides have been identified. Histatins
- 123. 123 Defensins Adaptive and innate immune response. Two families:- • Alpha-defensins = produce by PMNs. • Beta-defensins = produce by epithelial cells.
- 124. 124 Novel technologies such as 1. lab-on-a-chip and 2. microfluidic devices Advantages :- 1. The portable, 2. less training 3. easy-to-use diagnostic tools, 4. accurate 5. real-time assessment 6. disease-risk profile, 7. current disease activity and 8. response to therapeutic interventions. 9. cost-effective healthcare delivery. Disadvantages:- 1. Human error. 2. Incorrect interpretation. Rapid point-of-care diagnostics for periodontal disease GiannobileWV, BeiklerT, Kinney JS, RamseierCA, MorelliT, WongDT. Saliva as a diagnostictoolfor periodontal disease:currentstate and futuredirections. Periodontol2000.2009;50:52-64.
- 126. Dry mouth (xerostomia) is a subjective sense of dryness which may be due to: 1) Reduced salivary flow (hyposalivation) 2) Changed salivary secretion. Main causes of dry mouth 1) Medications. 2) Cancer treatments. 3) Salivary disease. 4) Dehydration. 5) Psychogenic. Dry mouth (xerostomia and hyposalivation) SugiyaH. (2014)Xerostomia.ReferenceModule in BiomedicalSciences. Elsevier.15-Oct-14
- 127. 127 Medications with a reported incidence of xerostomia 1. Anticholinergic agents: Atropine,Scopolamine 2. Antidepressant and antipsychotic agents: Imipramine,Amitriptyline,Clozapine 3. Diuretics: Furosemide 4. Antihypertensive agents:Captopril, Enalapril 5. Antianxiety agents: Benzodiazepines 6. Antihistamines: Astemizole, Loratadine, Brompheniramine
- 128. Swedish ophthalmologist HenrikSjögren in 1930. This includes:- 1. Connective tissue disorder 2. Keratoconjunctivitis 3. Xerostomia It commonly affects the salivary and lacrimal glands, resulting in xerostomia and dry eyes (keratoconjunctivitis sicca). PrimarySS- no other autoimmune disease is present, and SecondarySS- additional connective tissue diseases are present, such as rheumatoid arthritis, scleroderma. Sjögren’s Syndrome
- 129. 129 Difficulty in swallowing- especially in eating dry foods, such as biscuits (the cracker sign). Difficulty in controlling dentures. Difficulty in speaking. Mouth soreness. Unpleasant taste or loss of sense of taste. A dry mucosa– the lips adhere one to another and dental mirror may stick to the mucosa. Lack of the usual pooling of saliva in the floor of the mouth. Characteristic lobulated tongue, usually red, with partial or complete depapillation. CLINICAL FEATURES
- 130. 130 ORALCOMPLICATIONS Halitosis (oral malodour). Dental caries. Burning sensation. Intolerance of acids and spices. Taste changes.
- 131. 131 SALIVARY FLOW RATE INXEROSTOMIA 1. Unstimulated saliva flow rate Unstimulated whole saliva flow rate exceeds 1.5 mL/15 min (0.1 mL/min). A resting secretion rate of < 1.5 mL in 15 min indicates hyposalivation. 2. Stimulated saliva flow rate In normal persons the flow should well exceed 1 mL/min. A flow of < 0.5 mL in 5 min or < 1 mL in 10 min is decreased.
- 132. Diagnosis of xerostomia Sugiya H. (2014) Xerostomia.ReferenceModulein Biomedical Sciences.Elsevier.15-Oct-14
- 133. 133 10 steps to manage dry mouth 1. Sip on juices and other fluids throughout the day. 2. Replace missing saliva with salivary substitutes. 3. Stimulate saliva with sugar-free chewing gums. 4. Avoid spicy or dry foods or hard crunchy foods. 5. Always take water or non-alcoholic drinks with meals. 6. Avoid anything that may worsen dryness, such as: drugs, mouth- breathing habit. 7. Protection against dental caries. 8. Protect against halitosis. 9. Protect the lips with a lip salve. 10. Consider a humidifier for the room.
- 134. Sialorrhea is drooling or excess saliva that cannot be controlled. Caused by medication, psychiatric disorders. Major Medications group are Sialagogue drugs. Lespargot et al. indicated that drooling is related to one or more of three abnormalities. 1. Incomplete lip closure during swallowing. 2. Low suction pressure. 3. Prolonged delay between the suction and the swallowing. 134 Sialorrhea
- 135. Sialagogue drugs are substances designed to stimulate salivary secretion. These drugs act upon different receptor groups: 1. Direct and indirect muscarinic agonists. 2. Peripheral adrenergic α2 antagonists. (Yohimbine) 135 Sialagogue drugs
- 136. Parasympathomimetic drugs Muscarinic agonists mimic the action of acetylcholine on muscarinic receptors and cause increased secretion from exocrine glandular tissues. Divide into two groups: Muscarinic agonists Bui T, DuongH. Muscarinic Agonists.[Updated2023Apr 26] Direct agonist Indirect agonist. Bethanechol (5-10mg tab) Neostigmine (15-30mg) Carbachol (0.25-0.5mg) Physostigmine (60-240mg) Inj – 1-5mgSC or IM Pilocarpine (5 to 10 mg)
- 137. 137 Treatment Pharmacological therapy 1. Atropine- administered sublingually has the capacity to reduce drooling. 2. Scopolamine -applied through transdermal patches. 800 µg dose administered two/ three times a day. Minimally invasive methods Botulinum toxin injection- it acts by blocking the release of acetylcholine neurotransmitter. Photocoagulation of the salivary gland ducts. Concept of laser photocoagulation is based on the partial destruction of the gland. Surgical methods Neurectomy-Sectioning of the parasympathetic nerve reduces the flow of saliva. The tympanic plexus nerve and the tympanic cord may be sectioned.
- 138. Sialadenitis is the inflammation of the salivary gland. Caused by obstruction and infection by bacteria. Microorganisms involved are staphylococcal bacteria. Treatment includes antibiotics for bacterial infections, oral hydration, warm compression, and drugs that induce salivary secretion. 138 Sialadenitis
- 139. Mumps infection – caused by the paramyxovirus. Causes painful swelling of the parotid glands in childhood. Bilateral manifestation of the disease, with painful swelling to both glands. There are usually systemic signs of infection such as 1. Erythema (redness around the area), 2. Malaise (generalized weakness), 3. Tenderness, and 4. Fever. Mumps vaccine given with measles and rubella vaccinations during routine vaccination programs. Parotid gland inflammation (Parotitis)
- 140. 140 Sialolithiasis Sialolithiasis is a benign condition caused when a stone or calculus is lodged in a salivary duct. Signs and symptoms include pain and swelling in the affected duct, particularly during and after eating. Ultrasound imaging is the first step in the diagnosis. MRI and sialography can be used for ductal obstruction. The goal of treatment is to increase saliva flow through the duct with oral hydration and drugs that induce salivary secretion. Surgical removal of the calculus is required for chronic sialolithiasis that has failed conservative treatment.
- 141. 141 80% to 90% of salivary stones are found in theWharton duct. 1)Wharton duct is longer and more vertically angulated compared to the parotid duct, which leads to increased salivary stasis. 2) Submandibular gland tissue is composed of mucinous and serous acini, which produce a more viscous fluid adding to the mechanical stasis caused by theWharton duct. 3)Antigravity drainage.
- 142. It is a benign, noninflammatory enlargement of the submandibular glands. Common in malnutrition, alcoholism, & diabetes patients. Bilateral involvement. There is no sex predilection, and the peak age incidence is between 30 and 70 years of age. The gland’s secretory granules can accumulate in acinar cells, which disrupt the glands secretion. Histologically, salivary glands show enlargement of the acini and increased granulation of serous cells; & in chronic disease there is acinar atrophy seen. Treatment - hydration, warm compression and massage, pain relief with analgesics, sialagogues. Sialadenosis
- 143. A traumatic injury can cause the formation of mucoceles. Tearing of the salivary gland resulting in spillage of mucins into the surrounding tissue. It is a bluish swelling and typically appears on the lower lip. In addition, a mucocele of the sublingual gland, known as a ranula, occurs on the floor of the mouth. Ranulas are relatively larger than mucoceles. In rare circumstances, they have been known to descend into the neck receiving the name of “plunging” ranulas. Usually, mucoceles are asymptomatic, but they must be excised if they are large enough. Mucoceles
- 144. A ranula is a pseudocyst caused by either :- a. The extravasation of saliva or b. The retention of mucous of the sublingual gland lacks epithelial lining hence differentiates from a cyst. Two types:-Simple or Deep. Simple ranulas are mucous retention cysts located deep to the floor of the mouth but remain above the mylohyoid muscle. Deep ranula occurs when the sublingual duct is leaking, and the collecting mucous through the mylohyoid muscle into the submental or lateral neck, forming a pseudocyst. Caused by local trauma that damages the sublingual gland allowing mucous to collect. The ranula presents as a fluctuant, swollen mass at the floor of the mouth with a bluish tint. If larger, this may lead to dysphagia, however, it is usually painless unless infected. Ranula
- 145. 145 Neoplasia Of all head and neck cancers a) 80% parotid gland b) 2% submandibular gland c) 3% to 4% sublingual gland The most common primary parotid tumor is pleomorphic adenoma. Adenoid cystic and mucoepidermoid carcinomas are the most common submandibular gland malignancies. Treatment course may include excision for benign tumors. Selective neck dissection and adjuvant radiation therapy for advanced tumor staging.
- 146. 80% of salivary tumors are seen in parotid gland. The most common primary parotid tumor is pleomorphic adenoma. The management of neoplasia of the parotid typically includes surgical resection. This can be of 2 types:- 1) Superficial parotidectomy – indicated in superficial lobe of parotid 2) Total parotidectomy – involves removal of as much of the parotid tissue medial and lateral to the facial nerve as possible. Parotidectomy
- 147. Parotid gland has a special place in the world of surgery. Because the facial nerve courses through the parotid gland. Identifying this nerve is crucial when performing surgical procedures in the gland to prevent injuries. Some landmarks commonly used to identify the facial nerve trunk include the:- 1. cartilaginous tragal pointer, 2. the tympanomastoid suture, 3. the posterior belly of the digastric muscle, 4. the styloid process, and 5. the retromandibular vein.
- 148. 148 A first line was marked from the tip of the mastoid process, running along the superior border of the Posterior belly of diagastric. Second line was drawn along the posterior border of the ramus. These two lines intersect with each other anteriorly, forming the apex of the triangle (angle a). The base of the triangle is formed by third line starting from the tip of the mastoid process, (angle b) running anteriorly, till it joins the second drawn line along the posterior border of the ramus (angle c). The Facial nerve is often found within this triangle just above the angle b formed by the 1st and the 3rd line. The mean distance of FNT from the angle b was 12.18 ± 2 mm within a range of 9–15 mm. BorleRM, Jadhav A, Bhola N, HingnikarP, GaikwadP. Borle'striangle: A reliableanatomical landmarkfor easeof identificationof facial nerve trunkduring parotidectomy.J Oral Biol Craniofac Res.2019 Jan-Mar;9(1):33-36. Borle's triangle
- 149. Tumor of parotid gland termed as “dumbbell” tumor. Tumor grow between the posterior aspect of the mandibular ramus and the stylomandibular ligament. This causes a narrow constricted portion with larger unrestricted portion on either side forming a dumbbell shaped. Dumbbell-shaped tumor
- 150. Excision of the submandibular gland Usually involves :- a) Electrocautery and b) Dissection. Structures most at risk of injury are 1. the facial artery and vein, 2. overlying marginal mandibular branch of the facial nerve, and 3. the hypoglossal and lingual nerves medially. Extraoral incision – placed at least 2cm below the lower border of mandible to avoid damage to nerve. 150
- 151. 151 Excise the sublingual gland Most commonly involves :- 1.Transoral electrocautery and 2. Blunt dissection. Structures most at risk of injury are the lingual nerve and Wharton's duct.
- 152. 152 Complications 1. Facial nerve injury – may be transient or permanent. 2. Hematoma formation. 3. Sialocele ( salivary fistula) – common following parotid surgery. 4. Frey’s syndrome- Auriculotemporal syndrome– m/c complication Results from reinnervation of sweat glands of the skin from parotid parasympathetics. Patients experience facial sweating and flushing. Treatment glycopyrrolate.
- 153. Summary 153 Knowledge of anatomy and physiology of salivary glands is essential to distinctly identify various associated conditions and salivary gland pathologies. Precise anatomical knowledge is also essential to plan out treatment strategies and alter the patients lifestyle. Saliva has an important role in patients quality of life. Dental professionals need to be aware of the problems that arise when there is an overproduction or underproduction of saliva, and also change in quality. Saliva plays a significant role in keeping the relationship between the host and oral microbiota. In conditions with salivary gland dysfunction, the natural balance of the oral microbiome is often disturbed, leading to risks of gingivitis, caries and fungal infection. Salivary biomarkers have diagnostic value by identifying patients with enhanced disease susceptibility, identifying sites with active disease, predicting sites that will have active disease in the future and ⁄ or monitoring the effectiveness of therapy.
- 154. 154 06 References:- TuckerAS, Miletich I (eds):SalivaryGlands. Development,Adaptations and Disease. FrontOral Biol. Basel, Karger, 2010, vol 14, pp 1–20. Antonio NanciTen cate’s oral histology development, structure and function 8th edi. KrishnaGarg BDChaurasia’s HUMANANATOMY for DentalStudentsThird Edition. RamacharSM, Huliyappa HA.Accessory parotid gland tumors.Ann MaxillofacSurg. 2012 Jan;2(1):90-3. doi: 10.4103/2231-0746.95334. PMID: 23483721; PMCID: PMC3591091.
- 155. 9/1/2023 155 Chason HM, Downs BW.Anatomy, Head and Neck, ParotidGland. 2022Oct 24. In: StatPearls [Internet]. Treasure Island (FL):StatPearls Publishing; 2023Jan–. PMID: 30480958. Grewal JS, JamalZ, RyanJ.Anatomy, Head and Neck,SubmandibularGland. [Updated 2022 Dec 11]. In: StatPearls [Internet].Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Grewal JS, Bordoni B, Shah J, et al.Anatomy, Head and Neck,SublingualGland. [Updated 2022Jul 18]. In: StatPearls [Internet].Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Lau,C., & McGurk, M. (2019). Embryology of theSalivaryGlands.Clinical Embryology, 165–168. Inderbir singh’s human embryology eleventh edition. IorgulescuG. Saliva between normal and pathological. Important factors in determining systemic and oral health.J Med Life. 2009Jul-Sep;2(3):303-7.
- 156. 156 ACatalán, M., Nakamoto,T., & E Melvin,J. (2009). The salivary gland fluid secretion mechanism.TheJournal of Medical Investigation, 56(Supplement), 192–196. Patil PB, Patil BR. Saliva:A diagnostic biomarker of periodontal diseases. J IndianSoc Periodontol. 2011 Oct;15(4):310-7. Bhattarai KR, Kim HR, Chae HJ. Compliance with Saliva Collection Protocol in Healthy Volunteers: Strategies for Managing Risk and Errors. Int J Med Sci. 2018 May 22;15(8):823-831. Khurshid, Z.; Zohaib, S.; Najeeb, S.; Zafar, M.S.; Slowey, P.D.; Almas, K. Human Saliva Collection Devices for Proteomics: An Update. Int. J. Mol. Sci. 2016, 17, 846. Miranda-Rius J, Brunet-Llobet L, Lahor-Soler E, Farré M. Salivary Secretory Disorders, Inducing Drugs, and Clinical Management. Int J Med Sci. 2015 Sep 22;12(10):811-24. Giannobile WV, Beikler T, Kinney JS, Ramseier CA, Morelli T, Wong DT. Saliva as a diagnostic tool for periodontal disease: current state and future directions. Periodontol 2000. 2009;50:52-64. Delli, K.,Spijkervet, F. K. L., Kroese, F.G. M., Bootsma, H., &Vissink,A. (2014). Xerostomia.Saliva:Secretion and Functions, 109–125.
- 157. 157