
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Giant cell tumor
Similar to Giant cell tumor (20)
More from anwaradil4
Recently uploaded
Recently uploaded (20)
Giant cell tumor
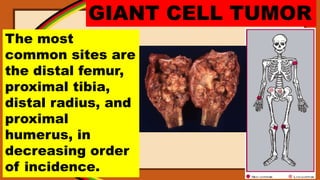
- 1. GIANT CELL TUMOR The most common sites are the distal femur, proximal tibia, distal radius, and proximal humerus, in decreasing order of incidence.
- 2. GIANT CELL TUMOR Involvement of the distal radius carries a more serious prognosis because most of these lesions are malignant.
- 3. GIANT CELL TUMOR The sacrum is the most common spinal site, representing 8% of cases. Giant cell tumor is the most common benign tumor of the sacrum.
- 4. GIANT CELL TUMOR Spinal sites above the sacrum are rare. Other infrequent sites are the calcaneus, innominate, rib, carpal bones, and patella.
- 5. GIANT CELL TUMOR Patellar neoplastic disease is uncommon; however, most patellar tumors are benign (73%) and are cartilaginous in origin (chondroblastomas or enchondromas) or giant cell tumors. Giant cell tumor is the most common neoplasm of the patella. Rarely, metastatic disease from any origin may affect the patella; this is the most common cause for malignancy in the patella.
- 6. GIANT CELL TUMOR Tumor usually begins in the metaphyseal end of a long bone in or adjacent to ossified epiphyseal line. It usually extends to the end of a long bone, abutting its joint surface, leaving the lesion subarticular.
- 7. GIANT CELL TUMOR The radiographic appearance of giant cell tumor is characteristic. It is an eccentric, metaphyseal, multilobed radiolucent lesion of a long bone. In an adult, it is located adjacent to the articular surface of the bone (subarticular).
- 8. GIANT CELL TUMOR It is also subarticular in flat bones, occurring near the sacroiliac joint and acetabulum in the innominate. Cortex is thinned and expanded, and endosteal margins show a wide zone of transition, suggesting a malignant lesion.
- 9. GIANT CELL TUMOR The lesion may traverse the entire shaft in a relatively thin bone, such as the fibula or ulna. A delicate periosteal reaction may develop, independent of infractions of cortex.
- 10. GIANT CELL TUMOR This sharply circumscribed lesion often expands bone, with a rather characteristic soap bubble pattern.
- 11. GIANT CELL TUMOR Most cases are purely lytic (60%), and the soap bubble pattern is present in 40% of cases. These bubbles and delineating lines are really reactive trabeculae of bone formed by appositional bone growth and do not actually chamber the lesion because of their peripheral location. Thus the giant cell tumor, removing numerous trabeculae by its neoplastic growth, prompts reinforcement of the remaining trabeculae, resulting in the soap bubble pattern.
- 12. GIANT CELL TUMOR Involvement of flat bones, such as the ilium, rib, and sacrum, demonstrate the same roentgen appearance of an expanding, radiolucent, soap bubble lesion.
- 13. GIANT CELL TUMOR If the tumor is very aggressive, a purely lytic radiolucent lesion will be seen with cortical breakthrough and development of a soft tissue mass.
- 14. GIANT CELL TUMOR Spinal involvement above the sacrum with expansion and lytic destruction of a vertebral body or neural arch is usually called an osteoblastoma or ABC radiographically, before biopsy. Cervical and lumbar spine are the most common sites. Radiologist alone cannot predict with any accuracy whether the giant cell tumor is benign or malignant.
- 15. GIANT CELL TUMOR GCT may also have aggressive features, such as a wide zone of transition, cortical thinning, expansile remodeling, or even cortical bone destruction and an associated soft-tissue mass
- 16. GIANT CELL TUMOR GCT within an apophysis. Lytic lesion with a nonsclerotic margin in the greater trochanter. Expansile component with only a thin rim of peripheral cortex remaining. Pathologic analysis demonstrated a GCT. The greater trochanter is an epiphyseal equivalent, and GCT can occur in this location. When GCT affects an apophysis, it does not typically extend to the subchondral bone.