1. Abdominal
Tuberculosis
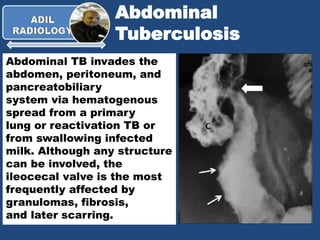
Abdominal TB invades the
abdomen, peritoneum, and
pancreatobiliary
system via hematogenous
spread from a primary
lung or reactivation TB or
from swallowing infected
milk. Although any structure
can be involved, the
ileocecal valve is the most
frequently affected by
granulomas, fibrosis,
and later scarring.
2. Abdominal
Tuberculosis
TB peritonitis may develop causing ascites and omental
and peritoneal thickening. TB peritonitis is divided into three
forms: wet, fibrotic, and dry. Wet peritonitis is characterized
by a large amount of viscous ascetic fluid (90 % of cases).
Fibrotic peritonitis is characterized by large omental masses
and intestinal adhesions, causing the omentum to form a hard
mass on palpation. Dry or plastic peritonitis is characterized
by fibrous peritoneal reaction, dens adhesions, and caseous
nodules.
3. Abdominal
Tuberculosis
Thickened peritoneum may be seen as a tiny
nodules or a thick nodular line surrounding
the viscera beneath the abdominal walls, with
marked enhancement after contrast injection.
5. Abdominal
Tuberculosis
TB ascitic fluid with septations is seen in
30–100 % of cases. The fluid typically has
attenuation between 25 and 45 HU, which
may reflect its exudative nature.
8. Abdominal
Tuberculosis
In Bauhin ’s ileocecal valve
syndrome , the CT show
hypertrophic ileocecal valve
with dilated small bowel loops
proximally. The absence of
abnormal contrast
enhancement, pathologic
intestinal manifestations, and
ileocecal mass are supportive
signs that assist in establishing
the diagnosis. Definite
diagnosis requires colonic
biopsy that typically shows
hypertrophic muscularis layer
with absence of inflammatory or
malignant changes.