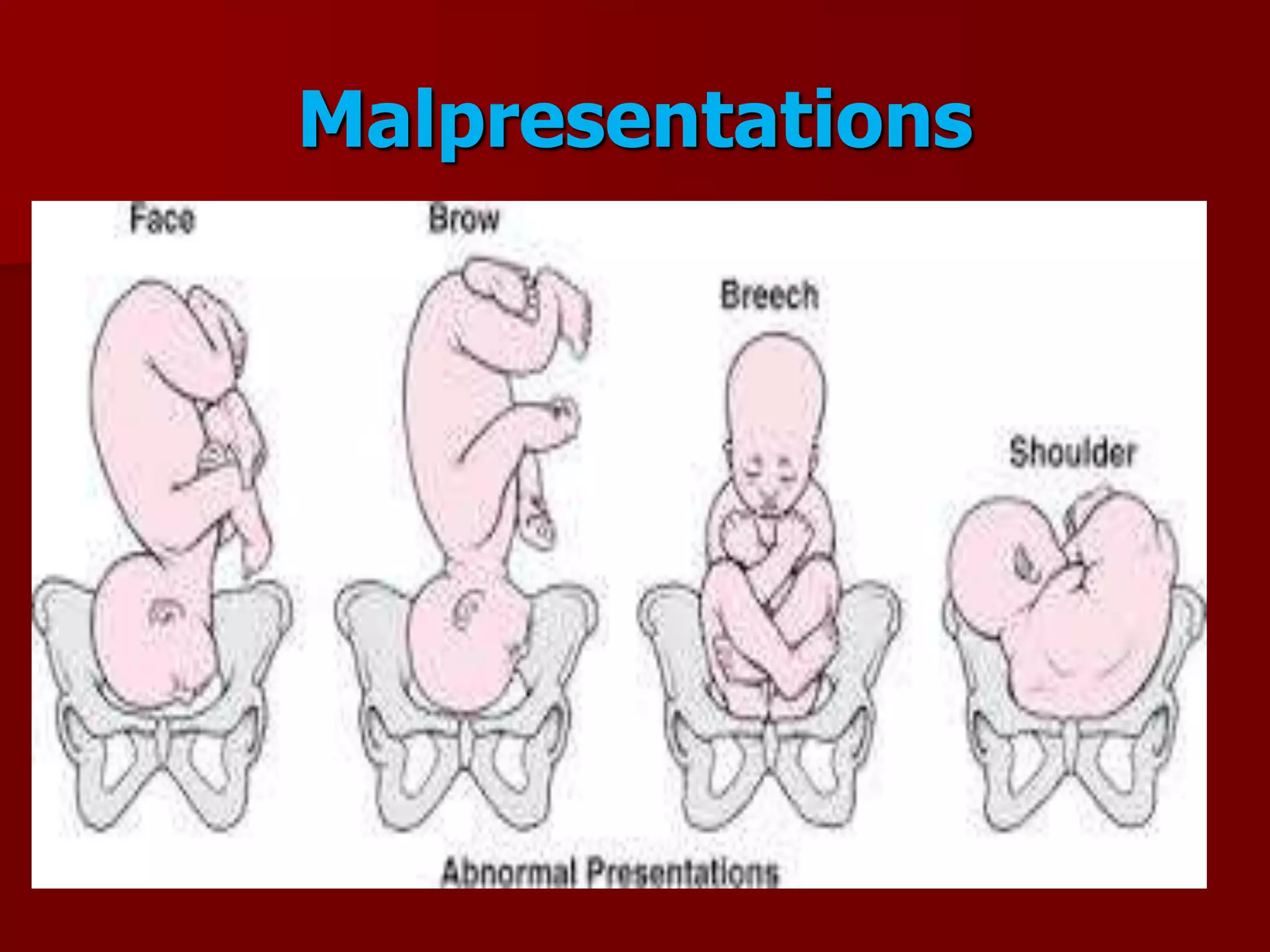
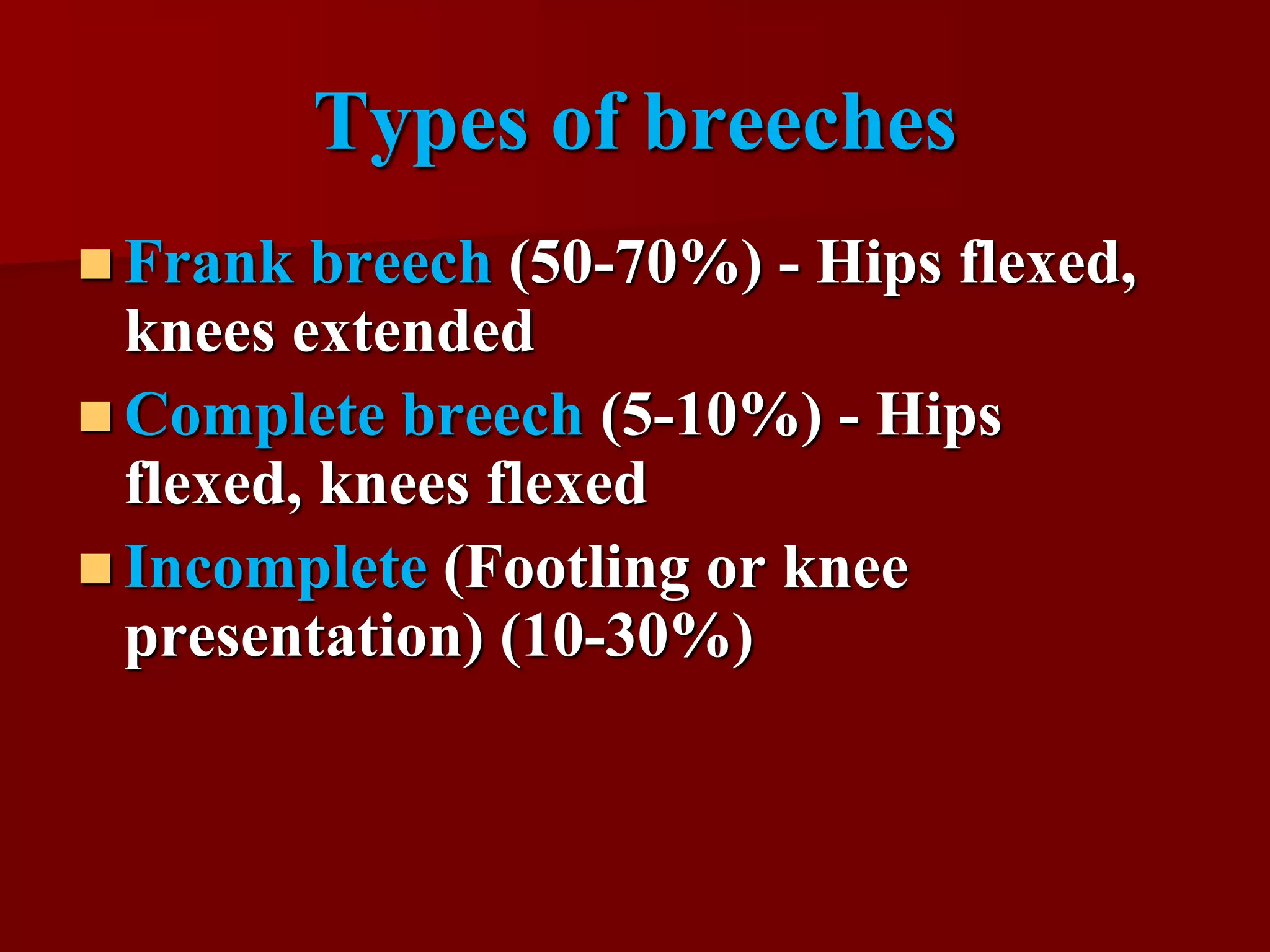
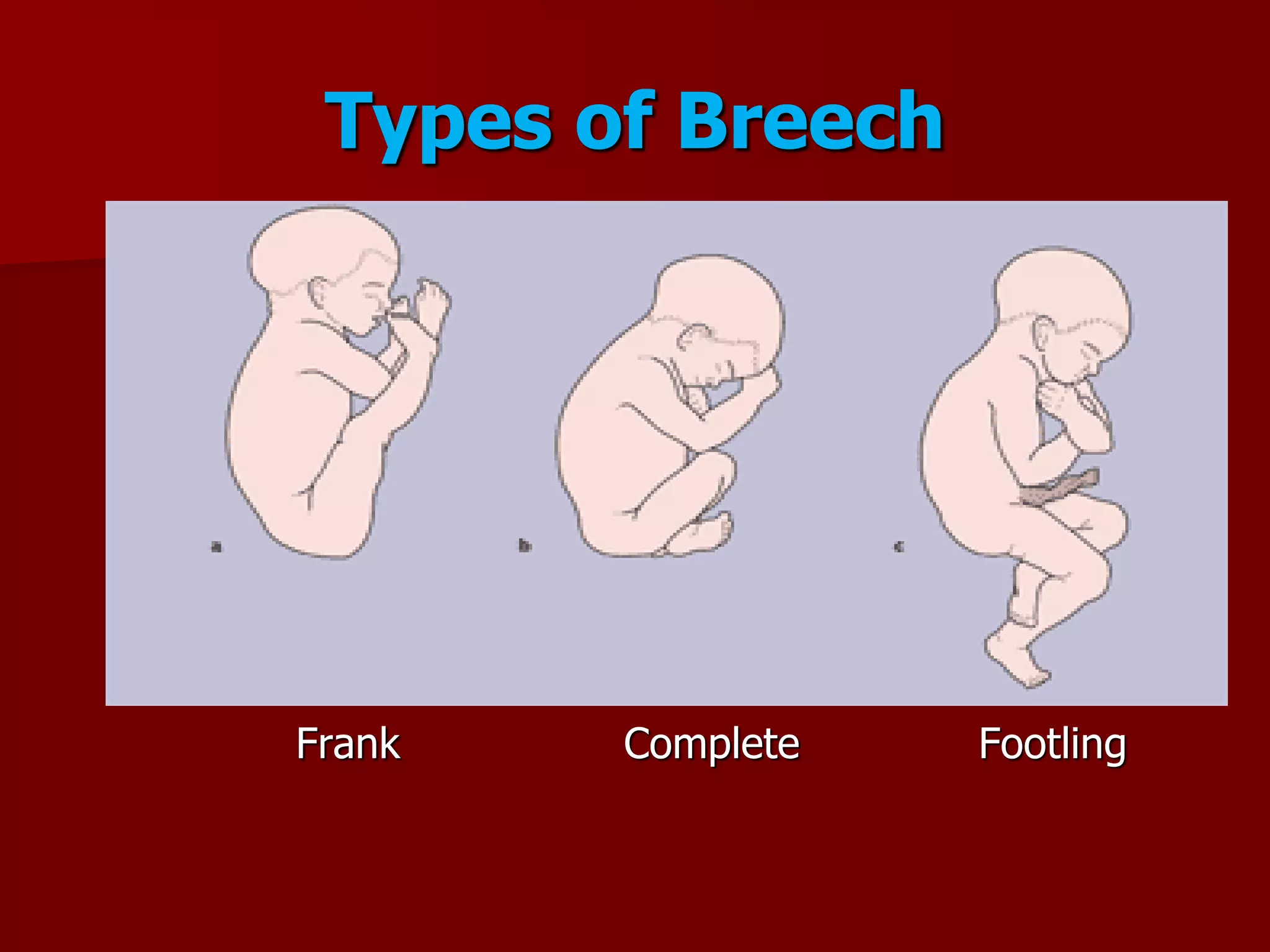
This document discusses breech presentation and external cephalic version. It defines breech presentation as one where the fetal buttocks present at the pelvic inlet. It describes the types of breeches including frank, complete, and footling. It discusses the diagnosis, management during pregnancy including external cephalic version, and complications of breech delivery. It then discusses transverse lie and unstable lie, their causes, diagnosis, and management including external cephalic version to correct the presentation. Finally, it provides details on performing external cephalic version including indications, technique, risks, and contraindications.