1. +
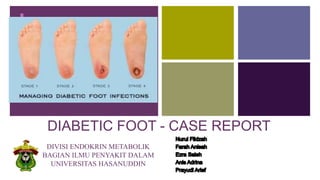
DIABETIC FOOT - CASE REPORT
DIVISI ENDOKRIN METABOLIK
BAGIAN ILMU PENYAKIT DALAM
UNIVERSITAS HASANUDDIN
2. +
Case
Name : Ny. M
Date of birth : 12-04-1969 / 40 years old
Gender : Female
Marital status : Married
Religion : Muslim
Address : Benteng, Wara
Timur
Medical Record Number : 010430
Date of Admission : 28-10-
2019
3. + History Taking
The patient notice a spontaneous small opening and redness without any external
injury on the dorsal and plantar aspect of left foot 2 weeks prior to admission.
Wound was painfull, swelling and spreading. Currently there is mild discharge on
the wound without foul smell. History of intermittent fever, nausea, vomiting, cough,
difficulty in breathing and sleeplessness was present.
There was history of amputation of little finger of the left hand a year ago due to
ischemic and heel of right foot in 2012.
Chief complaint: Injury of left foot
4. + History Taking
She was diagnosed with Type 2 Diabetes Mellitus 10 years ago,
uncontrol.
There’s no history and current impaired vision,
She was diagnosed with hyperurecemia, uncontrol.
The patient denied any history of heart disease, hypertention,
hypercholestrolemia.
There is no history of cigarette smoking.
5. +
Patient Status
General condition : Moderate Illness/Compos Mentis (E4M6V5)
Height : 159 cm
Weight : 53 kg
BMI : 23.34 kg/m2
Vital Sign
Blood pressure : 120/70 mmHg Heart rate : 75 x/minutes
Respiratory rate : 18 x/minutes Temperature : 37,3 ‘C
Physical Examination
7. +
Physical Examination
Neck
Lymph nodes : Enlargement (-)
Thyroid Gland : Enlargement (-)
JVP : R+ 2 cm H2O
Blood Vessels : In normal Range
Nuchal Rigidity : Negatif
Tumor : Negatif
Trachea : Deviation (-)
Toraks
Inspection : Symetrical left = right
Palpation : mass (-), vocal fremitus is
normal
Percussion: Sonor
Auscultation: breath sound : vesicular. Ronchi and
wheezing (-)
8. +
Physical Examination
Cor
Inspection: Ictus cordis isn’t visible
Palpation : Ictus cordis isn’t palpable, Thrill (-),
Tenderness (-)
Percussion :
Right Upper border 2nd ICS linea parasternalis dextra
Left Upper border 3th ICS llinea parasternalis sinistra
Right lower border 4th ICS linea parasternalis dextra
Left lower border 6th ICS linea axillaris anterior sinistra
Auscultation: Heart sound I/II pure regular, murmur (-
)
Abdomen
Inspection : convex, following breath
movement
Auscultation: Peristaltic sound (+),
normal
Palpation : Mass (-), tenderness (-),
there are no palpable
Percussion : Timpani (+), ascites (-)
9. +
Physical Examination
Lower extremities
Inspection : Ulcer on the left little toe 1x1cm.
Gangrene on the left fourth and little toes
(plantar pedis). Pus (-) , blood (-).
Palpation : Tenderness
Upper extremities
Inspection : Amputated left little finger.
Palpation : Tenderness (-)
18. Definition
• Diabetic foot is one of the most significant and devastating complications of
diabetes, and is defined as a foot affected by ulceration that is associated with
neuropathy and/or peripheral arterial disease of the lower limb in a patient with
diabetes.
19. Epidemiology
• Systematic review included a large sample of studies involving more than 800,000 global participants from
67 studies in the past three decades. These studies included patients from five continents.suggested that
the pooled prevalence of diabetic foot ulceration was about 6.3% worldwide
• The results suggested that the highest prevalence of diabetic foot ulceration was reported in North Americ
(13.0%), and the lowest prevalence was reported in Oceania (3.0%). The prevalence of diabetic foot ulcer
was relatively higher in Africa (7.2%) than in Asia (5.5%) and Europe (5.1%).
Zhang, P., 2017. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Annals of Medicine, 1, 1.
20. Clinical Manifestasions
Clinical manifestations of DM are associated
with the metabolic consequences of insulin
deficiency:
• Fasting sugar levels are not normal.
• Poliuria
• Polidipsia
• Polifagia
• Weight Loss
• Tired and sleepy
• Other symptoms that are complained of are tingling,
itching, blurred eyes, impotence in men, and prurity vulva
in women.
21. In addition, there are other
clinical symptoms that show
more signs of ulcers due to
microangiopathy in people with
diabetes mellitus, which is 5P
which means:
a. Pain(nyeri)
b. Paleness(kepucatan)
c. Paresthesia (kesemutan)
d. Pulselessness (denyut nadi
hilang)
e. Paralysis (kelumpuhan)
Clinical Symptoms
26. The nylon monofilament test is a
simply performed office test to
diagnose patients at risk for
ulcer formation due to
peripheral sensory neuropathy.
The test is abnormal if the patient
cannot sense the touch of the
monofilament when it is pressed
against the foot with just enough
pressure to bend the filament
27. DM Therapy: Non Pharmacology
•The course of the disease, the need for ongoing control and monitoring
DM complications, risk factors, non-pharmacological interventions,
pharmacological, and treatment targets
How to monitor blood glucose and interpret the results, recognize early
symptoms and manage hypoglycemia
The importance of foot care and regular physical exercise
Education
•Cannot walk barefoot
Check the foot every day, report to the doctor for skin peeling, redness, or
sores
Check footwear from foreign objects before use
Keep feet clean
Cut nails regularly
Dry regularly after the bathroom
Use cotton socks
Thin the callus regularly
Use custom made footwear
Feet Care
28. DM Therapy: Non Pharmacology
KARBOHIDRAT
•Karbohidrat: 45-
65%, berserat
tinggi, tidak boleh
& 130 g
•Glukosa dalam
bumbu masih
diperbolehkan
•Sukrosa <
5%
•Pemanis alternatif
•Makan tiga kali
sehari + selingan
LEMAK
•20-25% (Lemak
jenuh & 7%; lemak
tidak jenuh ganda
< 10%;
selebihnya lemak
tidak jenuh
tunggal)
•Batasi daging
berlemak dan
susu fullcream
(lemak trans)
•Konsumsi
kolesterol &200
mg/hari
PROTEIN
•10-20%
•Nefropati diabetik:
10% atau 0.8
g/kgBB dengan
65% diantaranya
bernilai biologik
tinggi
•Penderita DM
yang menjalani
HD: 1-1.2
g/kgBB/hari
NATRIUM
•2300 mg/hari
SERAT
•20-35 g/hari
•Kacang-kacangan,
buah, dan
sayuran,
karbohidrat tinggi
serat
PEMANIS
ALTERNATIF
•Berkalori: Hitung
kandungan
kalorinya (isomalt,
lactitol, maltitol,
mannitol, sorbitol,
xylitol)
•Fruktosa tidak
dianjurkan
Meningkatkan
kadar LDL.
Namun tidak ada
alasan
menghindari
makanan seperti
buah/sayur karena
mengandung
fruktosa alami
•Tak berkalori:
Aspartam, sakarin,
acesulfame
potassium,
sukralose,
neotame
29. DM Therapy: Non Pharmacology
• 3-5 kali per minggu
• 30-45 menit (total 150 menit per minggu)
• Jeda antar latihan tidak lebih dari 2 hari berturut-turut
• GDS < 100 mg/dl Konsumsi karbohidrat terlebih
dahulu
• GDS > 250 mg/dl Tunda olahraga
• Latihan jasmani bersifat aerobik
• Intensitas sedang
• Jalan cepat
• Bersepeda santai
• Jogging
• Berenang
• DM tanpa kontraindikasi (OA, HT tidak terkontrol,
retinopati, nefropati)
• Resistance training (latihan beban) 2-3 kali/minggu
Exercise
32. Yale Protocol (Insulin Drips)
Initial insulin
therapy (GDS 423):
Rapid-acting
insulin 5U / hour /
Syringe Pump
GDS 450-549 = 5 Units / hour / drips
GDS 350-449 = 4 Units / hour / drips
GDS 250-349 = 3 Units / hour / drips
GDS 150-249 = 2 Units / hour / drips
GDS 100-149 = 1 unit / hour / drips
-Target reduction in GDS from 50 to 100 mg / dL / hour
- If it does not reach the target, the dose is increased
50% from the initial dose.
- If the reduction in GDS is more than 100 mg / dL,
decrease the dose by 50% from the start.
- If GDS <80 stops insulin + bolus dextrose 40% 2
flacon (50 cc) in a 0.9% NACL infusion.
- If GDS 80-99 stops insulin + bolus dextrose 40%
25cc
33. Parameter Target
BMI (kg/m2) 18.5 - < 23*
Systolic Pressure (mmHg) < 140
Diastolic Pressure (mmHg) < 90
GDP (mg/dl) 80-130**
GD2PP (mg/dl) < 180**
HbA1c (%) < 7
LDL Cholesterol (mg/dl) < 100 or < 70 if
high risk for CVD
HDL Cholesterol (mg/dl) Men : > 40
Women: > 50
Trigliseride (mg/dl) < 150
*The Asia-Pacific Perspective: Redefining Obesity and Its
Treatment, 2000
**Standards of Medical Care in Diabetes, ADA 2015
Therapy
Goals