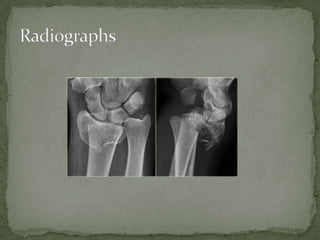
A 68-year-old female presented after falling and injuring her left wrist while getting out of the shower. On examination, she had obvious swelling and deformity of the right wrist with limited range of motion. X-rays revealed a distal radius fracture with dislocation of the radiocarpal joint, known as a dorsal Barton's fracture. Treatment would involve pain control, closed reduction of the fracture under sedation, and orthopedic consultation as non-operative treatment often fails for this type of injury.