
Recommended
More Related Content
Similar to Arrythmias Guide
Similar to Arrythmias Guide (20)
More from Safoora Qureshi
More from Safoora Qureshi (18)
Recently uploaded
Recently uploaded (20)
Arrythmias Guide
- 1. Arrythmias Prepared by: Mrs. Safoora Qureshi Nursing Instructor PIMS, Islamabad
- 3. Rhythm • Heart rate is the number of times the heart beats in a minute. • Heart rhythm is the pattern of the heart beat • It may be referred to as regular, irregular, fast or slow. • The normal heart rhythm is called sinus rhythm. • Arrhythmia: • a variation in the rhythm of the heartbeat • Dysrhythmia: • an unusual rhythm, either in electrical impulses or in speaking • Arrhythmia VS Dysrhythmia: • Both refer to an abnormal rhythm of the heart beat. • Dysrhythmias present with irregular heart beat, but still
- 4. MECHANISMS OF DYSRHYTHMIAS Normally the main pacemaker of the heart is the SA node, which spontaneously discharges 60 to 100 times per minute • Disorders of impulse formation can cause dysrythmies. Secondary pacemakers may originate from the AV node or Bundle of His or Purkinje system. • Secondary pacemakers can originate when they discharge more rapidly than the normal pacemaker of the SA node • Triggered beats (early or late) may come from an ectopic focus (area outside the normal conduction pathway) in the atria, AV node, or ventricles.
- 5. What is the rhythm of an ECG? • Sinus rhythm refers to the origination of the electrical activity coming from the sinoatrial node, or SA node • The first ECG strip shows a P wave with sinus morphology, thus normal sinus rhythm.
- 6. Causes of Arrythmias: • Coronary artery disease. • Irritable tissue in the heart (due to genetic or acquired causes). • Hypertension • Cardiomyopathy • Valve disorders. • Electrolyte imbalances in your blood, such as sodium or potassium imbalances. • Injury from a heart attack. • The healing process after heart surgery. • Other medical conditions.
- 7. Risk Factors: • Advancing age: age of 60 are more likely to develop dysrhythmia. • Congenital heart defects: • Family history: • Previous heart attacks or surgeries:
- 8. Symptoms: vary from silent to severe. • Chest pain or tightness • Dizziness or lightheadedness • Fainting /Syncope • Palpitation – a feeling of skipped heart beats or fluttering • Pounding in the chest • Shortness of breath • Weakness or fatigue
- 9. Diagnosis: • Electrocardiogram (ECG or EKG) • Holter monitor, is a portable ECG device • Event recorder, is a wearable ECG device • Echocardiogram • Implantable loop recorder
- 10. Types of Arrythmias 1. Tachyarrhythmia a. Supraventricular arrythmia • Atrial tachycardia: • Atrial fibrillation (A fib): • Atrial flutter: • Sinus Tachycardia • Junctional Dysrhythmias b. Ventricular arrythmia • Premature ventricular contractions(PVCs) • Ventricular tachycardia (VT): • Ventricular fibrillation (V-fib): 2. Bradyarrhythmia: • Sinus node dysfunction/Sinus brady arrythmia • Heart Block
- 11. Types of Arrythmias: 1. Tachyarrhythmia a. Supraventricular arrhythmias: • Arrhythmias that begin in the atria (the heart’s upper chambers). "Supra” means above. “Ventricular” refers to lower c ventricles. b. Ventricular arrhythmias: • Arrhythmias that begin in the ventricles (the heart’s lower chambers). 2. Bradyarrhythmia: • Slow heart rhythms that may be caused by disease in the heart’s conduction system, such as the sinoatrial (SA) atrioventricular (AV) node or HIS-Purkinje network
- 12. Supraventricular Arrythmias Paroxysmal supraventricular tachycardia (PSVT): • is a dysrhythmia originating in an ectopic focus, anywhere above the bifurcation of the bundle of His. • PSVT is a rapid rhythm that starts and stops suddenly. • The patient may feel palpitations, • dizziness, lightheadedness, or anxiety
- 13. Premature Atrial Contraction (PACs) • are extra heart beats that start in the upper chambers of the heart. • HR 60 to 100bpm, • ECG showed abnormal shape P wave Atrial tachycardia: • A rapid heart rhythm that starts in the atria. • ECG show inverted P
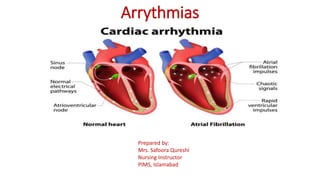
- 14. Atrial fibrillation (A fib): • Irregular heart rhythm, with a total disorganization of atrial electrical activity due to multiple ectopic foci resulting in loss of effective atrial contraction. • HR 350 to 600bpm. • ECG show fibrillatory (fib) waves. • May associated with CAD and RHD, HTN, and cardiac myopathy. Fib waves
- 15. Atrial flutter: • An atrial tachydysrhythmia, HR 250 to 350bpm • Identified by recurring, regular, sawtooth-shaped flutter waves (F)waves • Originate from a single ectopic focus in the right atrium. • May associated with CAD, HTN, and CLD
- 16. Sinus Tachycardia • The conduction pathway is the same as in normal sinus rhythm. • May associated Hard exercise, anxiety, certain drugs, or a fever • If there is no clear reason, called inappropriate sinus tachy • The heart rate might shoot up with just a little movement as a result of sympathetic nerve activation • HR >100 bpm with regular rhythm
- 17. Junctional Dysrhythmias. • The area of origin is the AV node, because; • The SA node has failed to fire or the signal has been blocked. • The AV node becomes the pacemaker of the heart • HR between 40-140bpm • Narrow QRS. • P waves may be hidden, inverted, retrograde, or short/upright.
- 18. Ventricular Arrythmias Premature ventricular contractions (PVCs): • is a contraction originating in an ectopic focus in the ventricle. • It is the premature occurrence of QRS complex, which is wide and distorted in shape. • PVCs may sensed as skipped beats. Because the ventricles are only partially filled, the PVC frequently does not generate a pulse. • Rate: Depends on rate of underlying rhythm • Rhythm: Irregular whenever a PVC occurs • P Waves: None associated with the PVC • PR Interval: None associated with the PVC • QRS: Wide (>0.10 sec), bizarre appearance
- 19. Ventricular tachycardia (VT): • It occurs when an ectopic focus or foci fire repetitively and the ventricle takes control as the pacemaker. • Rate: 100–250 bpm, • Rhythm: Regular • P Waves: None or not associated with the QRS • PR Interval: None • QRS: Wide (>0.10 sec), bizarre appearance Monomorphic VT Polymorphic VT
- 20. Ventricular fibrillation (V-fib): • is characterized by disorganized firing of impulses from the ventricles. • Chaotic electrical activity occurs with no ventricular depolarization • Mechanically the ventricle is quivering and no effective contraction and consequently NO CO • Represents the firing of multiple ectopic foci in ventricle. • This is a medical emergency that must be treated with CPR and defibrillation . Ventricular fibrillation
- 21. Bradyarrhythmia • Sinus node dysfunction: Slow heart rhythms due to an abnormal SA node Sinus bradycardia: • Has a normal sinus rhythm, but the SA node fires at a rate less than 60 beats/min & is referred to as absolute bradycardia. Heart block: • Heart block is a type of heart rhythm disorder (arrhythmia) • A delay or complete block of the electrical impulse as it travels from the sinus node to the ventricles. • The level of the block or delay may occur in • the AV node or HIS-Purkinje system. • The heartbeat may be irregular Rate: Slow (<60 bpm) Rhythm: Regular P Waves: Normal (upright and uniform) PR Interval: Normal (0.12–0.20 sec) QRS: Normal (0.06–0.10 sec) Sinus Bradycardia
- 22. Types / Degree of Heart Block First-degree (AV ) block. • This is the least severe type • AV) block is a condition of abnormally slow conduction through the AV node. • ECG changes include a • PR interval of greater than 0.20sec without disruption of atrial to ventricular conduction. • This condition is asymptomatic and discovered only on routine ECG. • There is no treatment for first- degree AV block.
- 23. Second-degree AV block. • The electrical signals between the atria and ventricles can intermittently fail to conduct Types of AV Block: Mobitz type I • The electrical signals get slower and slower between beats. • Over time the heart drops a beat and then the process repeats. Mobitz type II • A certain number of impulses from the SA node are not conducted to the ventricles. • No progressive slowing of the electrical signal. • AV block can often progress to third-degree heart block. P wave Missing QRS
- 24. • Third-degree Block (complete heart block). • Occur when there is no connection or dissociation of electrical activity from the atria and ventricles • This is the most severe type, with complete failure of electrical conduction. • The electrical signal from the atria to the ventricles is completely blocked • There is a This can result in no pulse or a very slow pulse if a backup heart rate is present.
- 25. Medical Management Antidysrhythmic Drugs: • Class I:Sodium channels blockers (decrease conduction velocity ). Procainamide, lidocaine, Propafenone • Class II: Beta- blockers (decrease automaticity in SA node, decrease conduction velocity in AV node). Atenolol, metoprolol • Class III: Potass ium channels blockers:(Delay repolarization). Amiodarone, Bretylium • Class IV: Calcium blockers (Decrease automaticity of SA node, delay AV node conduction).Verapamil, diltiazem • Other Antidysrhythmic Drugs. Adenosine, Digoxin,
- 26. Therapeutic techniques Vagal maneuvers: • Certain dysrhythmias, like SVT supraventricular tachycardia, can be stopped by using maneuvers that include holding your breath and straining, dunking your face in ice water or coughing. These actions affect the vagus nerves that control your hear Medication: • Adenosine (Adenocard) Adenosine is the first-line medical treatment for the termination of paroxysmal SVT.
- 27. Defibrillation Cardioversion / Defibrillation • For certain dysrhythmias – like atrial fibrillation – patient may treated with this procedure, during which a electric shock is delivered to your heart through paddles or patches on your chest. The current affects the electrical impulses and can restore a normal rhythm.
- 28. Invasive Procedures Catheter Ablation; • is a minimally invasive treatment for fast heartbeats. Catheter ablation is one type of heart ablation procedure used to treat abnormal heart rhythms (arrhythmias). Ablation is a technique used to strategically destroy abnormal tissue and restore proper function to the heart. • The procedure uses hot or cold energy to create scars in your heart tissue where the arrhythmia is occurring. The scars help block abnormal electrical impulses and prevent abnormal rhythms.
- 29. Device implantation: pacemaker or implantable cardioverter- defibrillator (ICD). A pacemaker is a small device placed under the skin near the collarbone in a minor surgical procedure. A wire extends from the device to the heart. If a pacemaker detects an abnormal heart rate, it emits electrical impulses that stimulate the heart to beat at a normal rate.
- 30. • Maze procedure: During this procedure, a surgeon makes a series of incisions in the upper half of the heart (atria) to create a pattern (or maze) of scar tissue to interfere with stray electrical impulses that cause some types of dysrhythmia. The procedure is very effective, but it is usually reserved for people who don’t respond to other treatments or for those who are having heart surgery for other reasons.
- 31. surgery • Coronary artery bypass grafting (CABG): This surgery improves blood flow to your heart by creating a bypass around your narrowed coronary arteries using arteries or veins taken from other parts of your body
- 32. Pacemaker
- 33. Pacemaker • A pacemaker is a small device that's placed (implanted) in the chest to help control the heartbeat. • It's used to prevent the heart from beating too slowly. Implanting a pacemaker in the chest requires a surgical procedure. • A pacemaker is also called a cardiac pacing device Causes: • Arrhythmias • Heart blocks • Heart failure. • Heart attack
- 34. Parts of Pacemaker • Pulse generator. This small metal container houses a battery and the electrical circuitry that controls the rate of electrical pulses sent to the heart. • Leads (electrodes). One to three flexible, insulated wires are each placed in one or more chambers of the heart and deliver the electrical pulses to adjust the heart rate. However, some newer pacemakers don't require leads. These devices, called leadless pacemakers, are implanted directly into the heart muscle.
- 35. Types • Single chamber pacemaker. This type usually carries electrical impulses to the right ventricle of heart. • Dual chamber pacemaker. This type carries electrical impulses to the right ventricle and the right atrium of your heart to help control the timing of contractions between the two chambers. • Biventricular pacemaker. Biventricular pacing, also called cardiac resynchronization therapy, is for people who have heart failure and heartbeat problems. This type of pacemaker stimulates both of the lower heart chambers (the right and left ventricles) to make the heart beat more efficiently.
- 36. Risk factors • Infection near the site in the heart where the device is implanted • Swelling, bruising or bleeding at the pacemaker site, especially if you take blood thinners • Thromboembolism near the pacemaker site • Damage to blood vessels or nerves near the pacemaker • Pneumothorax • Hemothorax • Movement (shifting) of the device or leads, which could lead to cardiac perforation (rare)
- 37. Monitoring of Patient after procedure • Continue ECG monitoring to evaluate the pacemaker status such as • Failure to sense ( pacer lead damage) • Failure to capture (battery failure) • Check vital signs • Observe complications such as; • infection, hematoma formation, pneumothorax • Perforation • Prophylactic antibiotics • Postinsertion x-rays to check lead placement • Limited arm and shoulder movement to prevent dislodgment of pacing lead
- 38. Home Care Teaching • Follow-up Care to insertion site • Report sign of infection • Keep incision side dry and clean and check for infection • Avoid lifting arm on pacemaker side above the shoulder • Avoid vigorous exercises for a period of time • Avoid direct blows to pacemaker side • Avoid close proximity to high-voltage electric generators, large magnetic such as MRI • Microwaves and cell phones are save but keep your cell 6inch away • Security alert system may interfere with pacemaker function • Wear Medic alert ID or pacemaker information card all the time